

Total Sleep Time in the Taiwan Obstructive Lung Disease Cohort
- PMID: 34281018
- PMCID: PMC8296961
- DOI: 10.3390/ijerph18137080
Total Sleep Time in the Taiwan Obstructive Lung Disease Cohort
Abstract
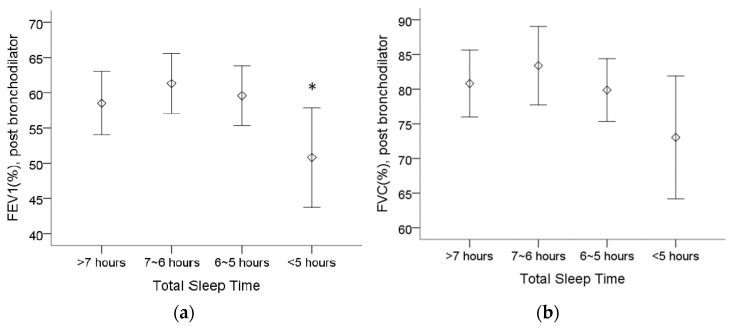
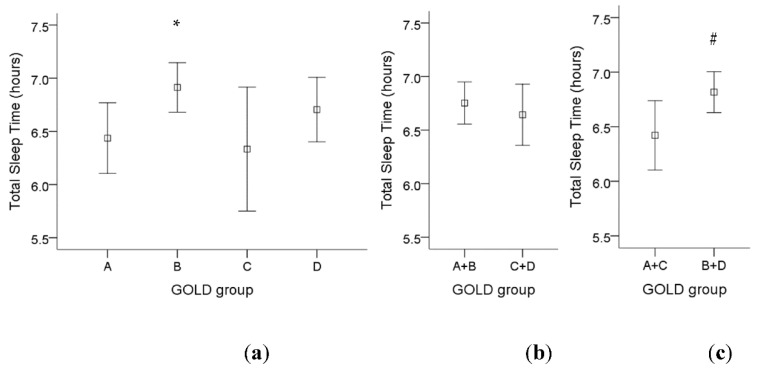
Patients with chronic obstructive pulmonary disease (COPD) have been reported to have poor sleep quality. However, total sleep time has not been evaluated in detail among patients with COPD. This retrospective, observational, multicenter research study was performed across six participating hospitals in Taiwan, with a total of 421 adult patients enrolled. Pulmonary function, the Modified British Medical Research Council Dyspnea Scale, the COPD Assessment Test and basic clinical data were assessed. The Pittsburgh Sleep Quality Index was also administered to patients, and the total sleep time was extracted for further analysis. The patients whose total sleep time was between 6 and 7 h had better pulmonary function, and the patients who slept less than 5 h had worse comorbidities. There was a significant higher total sleep time in Global Initiatives for Chronic Obstructive Lung Disease (GOLD) group B compared to GOLD group A. COPD patients who sleep between 5 and 6 h used fewer oral steroids and were less likely to use triple therapy (long-acting beta-agonist, long-acting muscarinic antagonist, inhaled cortical steroid). COPD patients sleeping from 5 to 7 h had better clinical features than those sleeping less than 5 h in terms of pulmonary function, comorbidities and medication usage.
Keywords: COPD; PSQI; comorbidity; pulmonary function; total sleep time.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
Similar articles
-
Factors responsible for poor sleep quality in patients with chronic obstructive pulmonary disease.BMC Pulm Med. 2016 Aug 8;16(1):118. doi: 10.1186/s12890-016-0281-6. BMC Pulm Med. 2016. PMID: 27501837 Free PMC article.
-
The relationship between sleep quality and functional exercise capacity in COPD.Clin Respir J. 2016 Jul;10(4):477-85. doi: 10.1111/crj.12249. Epub 2015 Jan 15. Clin Respir J. 2016. PMID: 25515647
-
Comorbidities in chronic obstructive pulmonary disease: Results of a national multicenter research project.Adv Clin Exp Med. 2019 Mar;28(3):319-324. doi: 10.17219/acem/78024. Adv Clin Exp Med. 2019. PMID: 30943332
-
Characteristics of Patients with Chronic Obstructive Pulmonary Disease at the First Visit to a Pulmonary Medical Center in Korea: The KOrea COpd Subgroup Study Team Cohort.J Korean Med Sci. 2016 Apr;31(4):553-60. doi: 10.3346/jkms.2016.31.4.553. Epub 2016 Mar 10. J Korean Med Sci. 2016. PMID: 27051239 Free PMC article.
-
Tiotropium bromide. A review of its use as maintenance therapy in patients with COPD.Treat Respir Med. 2004;3(4):247-68. doi: 10.2165/00151829-200403040-00005. Treat Respir Med. 2004. PMID: 15350163 Review.
Cited by
-
Poor sleep quality in chronic obstructive pulmonary disease.Tunis Med. 2025 Feb 5;103(2):255-259. doi: 10.62438/tunismed.v103i2.4680. Tunis Med. 2025. PMID: 40096727 Free PMC article. English.
References
-
- Fleetham J., West P., Mezon B., Conway W., Roth T., Kryger M. Sleep, arousals, and oxygen desaturation in chronic obstructive pulmonary disease. The effect of oxygen therapy. Am. Rev. Respir. Dis. 1982;126:429–433. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
