

High Oxalate Concentrations Correlate with Increased Risk for Sudden Cardiac Death in Dialysis Patients
- PMID: 34281958
- PMCID: PMC8729829
- DOI: 10.1681/ASN.2020121793
High Oxalate Concentrations Correlate with Increased Risk for Sudden Cardiac Death in Dialysis Patients
Abstract
Background: The clinical significance of accumulating toxic terminal metabolites such as oxalate in patients with kidney failure is not well understood.
Methods: To evaluate serum oxalate concentrations and risk of all-cause mortality and cardiovascular events in a cohort of patients with kidney failure requiring chronic dialysis, we performed a post-hoc analysis of the randomized German Diabetes Dialysis (4D) Study; this study included 1255 European patients on hemodialysis with diabetes followed-up for a median of 4 years. The results obtained via Cox proportional hazards models were confirmed by competing risk regression and restricted cubic spline modeling in the 4D Study cohort and validated in a separate cohort of 104 US patients on dialysis after a median follow-up of 2.5 years.
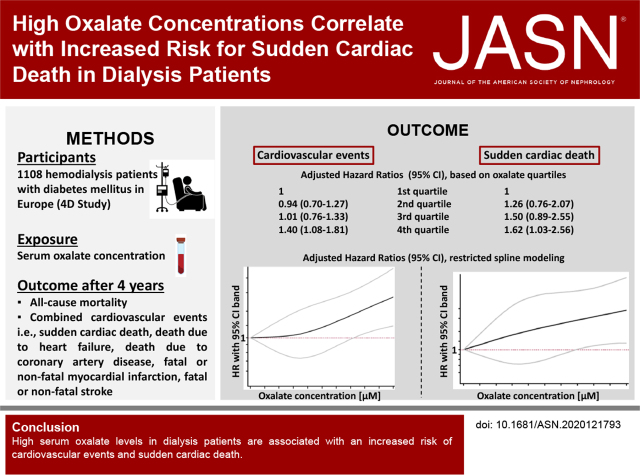
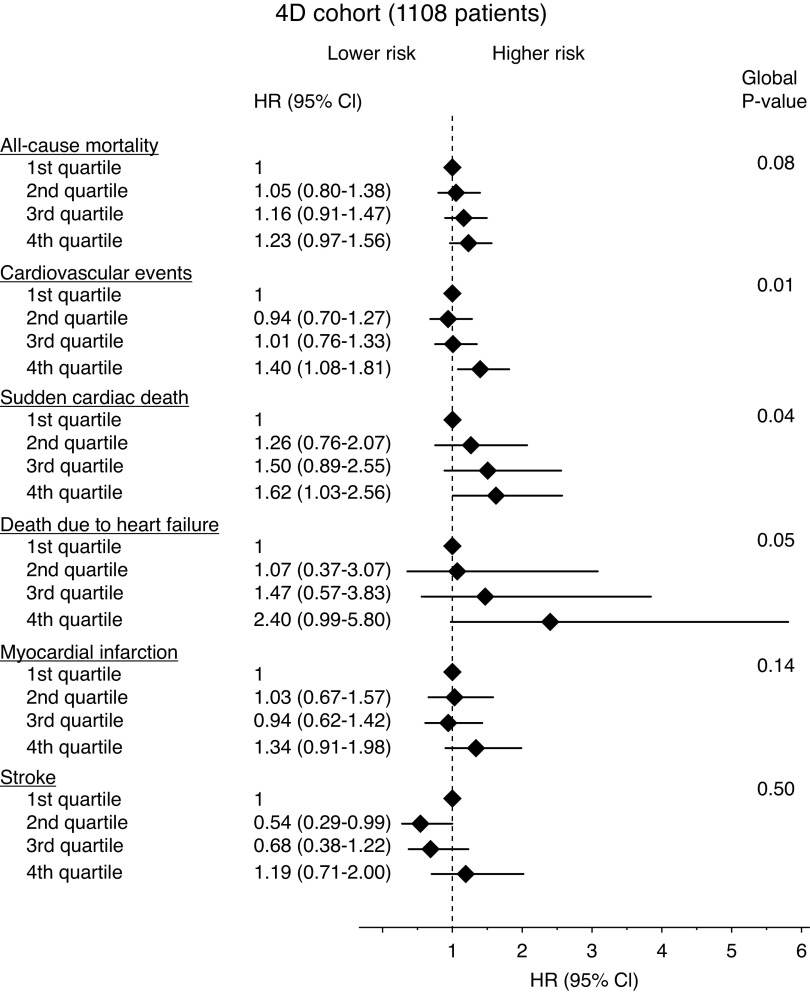
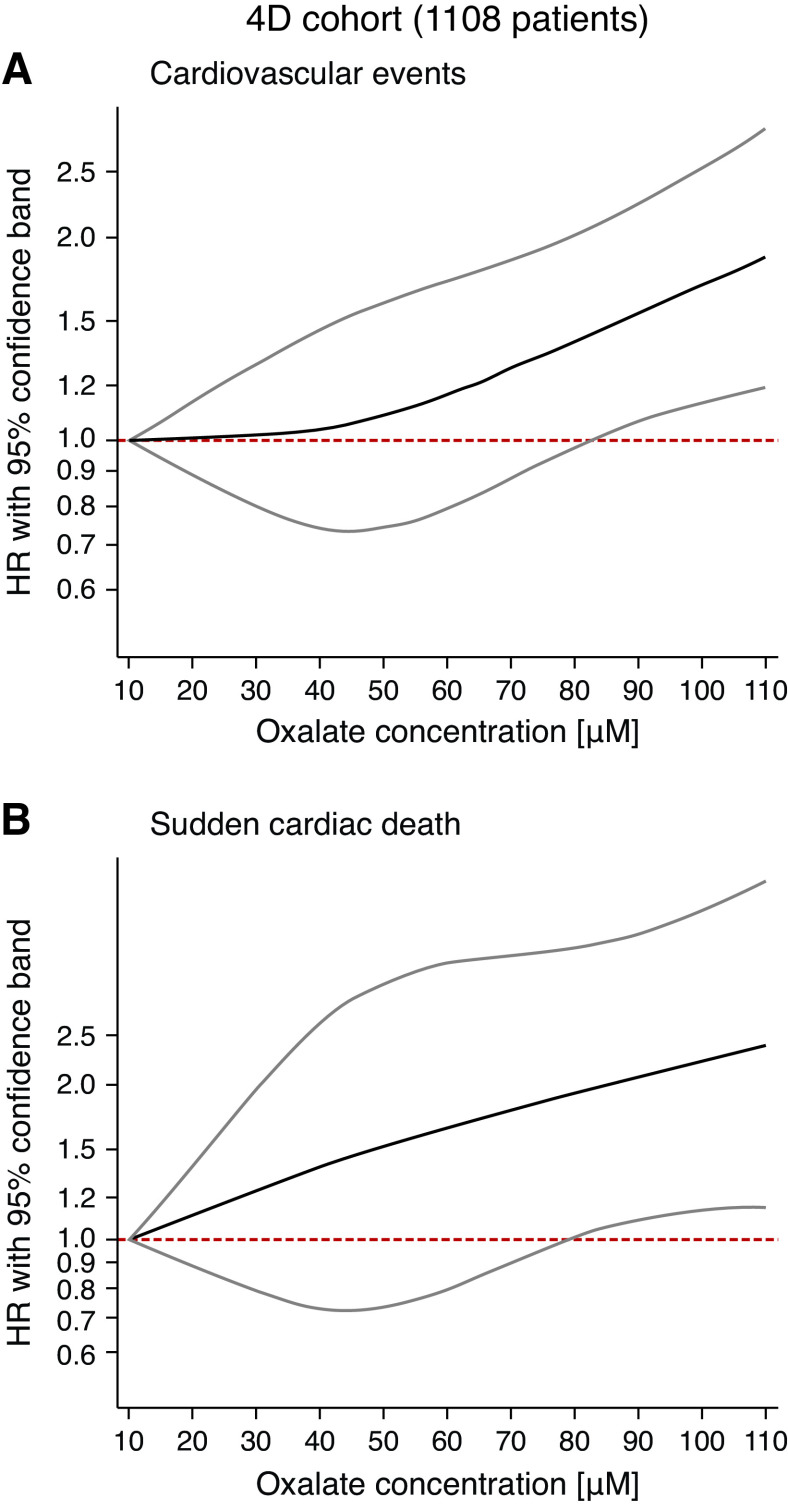
Results: A total of 1108 patients had baseline oxalate measurements, with a median oxalate concentration of 42.4 µM. During follow-up, 548 patients died, including 139 (25.4%) from sudden cardiac death. A total of 413 patients reached the primary composite cardiovascular end point (cardiac death, nonfatal myocardial infarction, and fatal or nonfatal stroke). Patients in the highest oxalate quartile (≥59.7 µM) had a 40% increased risk for cardiovascular events (adjusted hazard ratio [aHR], 1.40; 95% confidence interval [95% CI], 1.08 to 1.81) and a 62% increased risk of sudden cardiac death (aHR, 1.62; 95% CI, 1.03 to 2.56), compared with those in the lowest quartile (≤29.6 µM). The associations remained when accounting for competing risks and with oxalate as a continuous variable.
Conclusions: Elevated serum oxalate is a novel risk factor for cardiovascular events and sudden cardiac death in patients on dialysis. Further studies are warranted to test whether oxalate-lowering strategies improve cardiovascular mortality in patients on dialysis.
Keywords: cardiovascular disease; chronic hemodialysis; chronic kidney failure; oxalate; sudden cardiac death; uremic toxins.
Copyright © 2021 by the American Society of Nephrology.
Figures
Comment in
-
Authors' Reply: Calcium-Based Phosphate Binders and Plasma Oxalate Concentration in Dialysis Patients.J Am Soc Nephrol. 2022 Jul;33(7):1428. doi: 10.1681/ASN.2022030359. Epub 2022 May 2. J Am Soc Nephrol. 2022. PMID: 35500939 Free PMC article. No abstract available.
-
Calcium-Based Phosphate Binders and Plasma Oxalate Concentration in Dialysis Patients.J Am Soc Nephrol. 2022 Jul;33(7):1427. doi: 10.1681/ASN.2022030248. Epub 2022 May 2. J Am Soc Nephrol. 2022. PMID: 35500940 Free PMC article. No abstract available.
References
-
- van Walraven C, Manuel DG, Knoll G: Survival trends in ESRD patients compared with the general population in the United States. Am J Kidney Dis 63: 491–499, 2014 - PubMed
-
- Saran R, Robinson B, Abbott KC, Bragg-Gresham J, Chen X, Gipson D, et al. : US Renal Data System 2019 Annual Data Report: Epidemiology of kidney disease in the United States. Am J Kidney Dis 75[Suppl 1]: A6–A7, 2020 - PubMed
-
- Cheung AK, Sarnak MJ, Yan G, Berkoben M, Heyka R, Kaufman A, et al. ; HEMO Study Group: Cardiac diseases in maintenance hemodialysis patients: Results of the HEMO Study. Kidney Int 65: 2380–2389, 2004 - PubMed
-
- Chertow GM, Block GA, Correa-Rotter R, Drüeke TB, Floege J, Goodman WG, et al. ; EVOLVE Trial Investigators: Effect of cinacalcet on cardiovascular disease in patients undergoing dialysis. N Engl J Med 367: 2482–2494, 2012 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
