

Consensus disease definitions for neurologic immune-related adverse events of immune checkpoint inhibitors
- PMID: 34281989
- PMCID: PMC8291304
- DOI: 10.1136/jitc-2021-002890
Consensus disease definitions for neurologic immune-related adverse events of immune checkpoint inhibitors
Erratum in
-
Correction: Consensus disease definitions for neurologic immune-related adverse events of immune checkpoint inhibitors.J Immunother Cancer. 2021 Dec;9(12):1. doi: 10.1136/jitc-2021-002890corr1. J Immunother Cancer. 2021. PMID: 34907030 Free PMC article. No abstract available.
Abstract
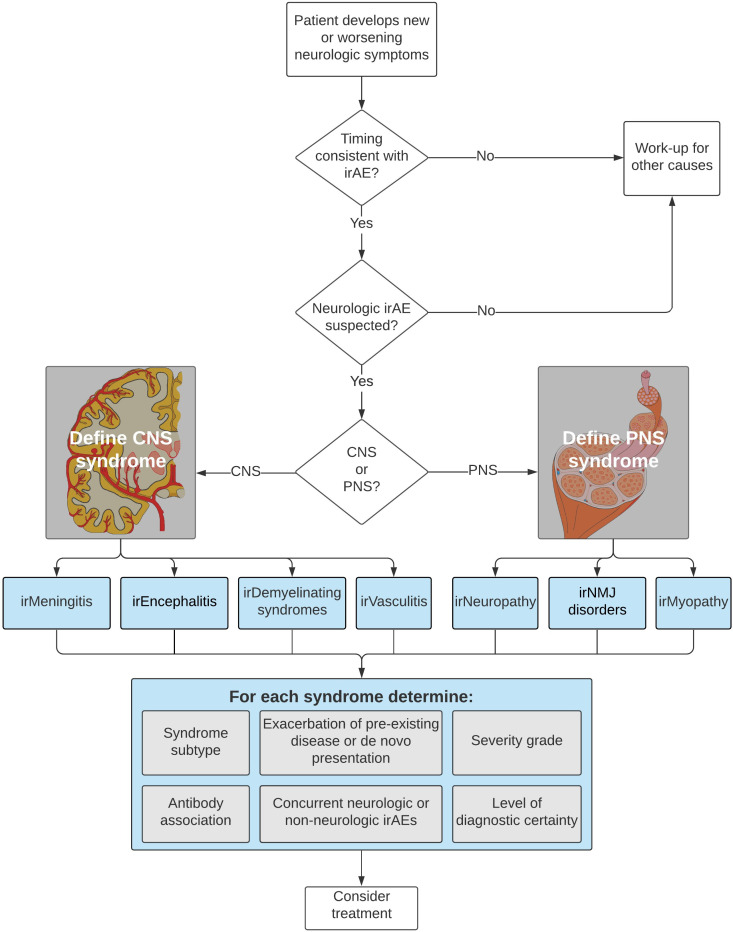
Expanding the US Food and Drug Administration-approved indications for immune checkpoint inhibitors in patients with cancer has resulted in therapeutic success and immune-related adverse events (irAEs). Neurologic irAEs (irAE-Ns) have an incidence of 1%-12% and a high fatality rate relative to other irAEs. Lack of standardized disease definitions and accurate phenotyping leads to syndrome misclassification and impedes development of evidence-based treatments and translational research. The objective of this study was to develop consensus guidance for an approach to irAE-Ns including disease definitions and severity grading. A working group of four neurologists drafted irAE-N consensus guidance and definitions, which were reviewed by the multidisciplinary Neuro irAE Disease Definition Panel including oncologists and irAE experts. A modified Delphi consensus process was used, with two rounds of anonymous ratings by panelists and two meetings to discuss areas of controversy. Panelists rated content for usability, appropriateness and accuracy on 9-point scales in electronic surveys and provided free text comments. Aggregated survey responses were incorporated into revised definitions. Consensus was based on numeric ratings using the RAND/University of California Los Angeles (UCLA) Appropriateness Method with prespecified definitions. 27 panelists from 15 academic medical centers voted on a total of 53 rating scales (6 general guidance, 24 central and 18 peripheral nervous system disease definition components, 3 severity criteria and 2 clinical trial adjudication statements); of these, 77% (41/53) received first round consensus. After revisions, all items received second round consensus. Consensus definitions were achieved for seven core disorders: irMeningitis, irEncephalitis, irDemyelinating disease, irVasculitis, irNeuropathy, irNeuromuscular junction disorders and irMyopathy. For each disorder, six descriptors of diagnostic components are used: disease subtype, diagnostic certainty, severity, autoantibody association, exacerbation of pre-existing disease or de novo presentation, and presence or absence of concurrent irAE(s). These disease definitions standardize irAE-N classification. Diagnostic certainty is not always directly linked to certainty to treat as an irAE-N (ie, one might treat events in the probable or possible category). Given consensus on accuracy and usability from a representative panel group, we anticipate that the definitions will be used broadly across clinical and research settings.
Keywords: autoimmunity; clinical trials as topic; guidelines as topic; immunotherapy; translational medical research.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: ACG has served on an advisory board and/or consulted with Alexion, Ra Pharma/UCB and Momenta pharmaceuticals/Janssen. She has received royalties from Oakstone Publishing and research support from the Myasthenia Gravis Foundation of America, the MG Rare Disease Network and Project Data Sphere® for an irAE-N registry. She has received clinical trial support to the institution from Ra Pharma and Momenta. LBB receives salary support from Biogen, royalties from Oakstone Publishing, and research support from Project Data Sphere for an irAE-N registry. BKC reports research support from Project Data Sphere for an irAE-N registry. JH receives research support from Project Data Sphere for an irAE-N registry and from GE Healthcare. THS is an employee at the not-for-profit corporation Project DS, with a trade name of Project Data Sphere. AAA served on medical advisory boards for Alexion, Sarepta, CSL Behring, Strongbridge Pharma, Argenx, Ra Pharmaceuticals, and as a neurology consultant for Johnson & Johnson COVID-19 vaccine trials. ABW served on a medical advisory board or as a consultant with Iovance, Novartis, Shanghai Jo’Ann Medical Technology. PKB has consulted for Angiochem, Genentech-Roche, Lilly, Tesaro, Voyager Therapeutics, ElevateBio, Pfizer (Array), Pfizer, SK Life Sciences and Dantari, received grant/research support (to Massachusetts General Hospital) from Merck, BMS and Lilly and honoraria from Merck, Pfizer, Genentech-Roche and Lilly. TAC has received royalties from Wolters Kluwer. SLC serves as the Editor of the Neurology®Podcast and Neurology Minute™. She has received research and/or clinical fellowship support from the Western Institute for Veterans Research, the Siegel Rare Neuroimmune Association, the Immune Deficiency Foundation, Alexion, the Barbara Gural Steinmetz Foundation, and the Sumaira Foundation for NMO. She has served on an advisory board and/or consulted with Alexion, Genentech, VielaBio, Guidepoint, Clarion Healthcare Consulting, ExpertConnect (majority fees paid to University of Utah). JC has received consulting fees from Sanofi-Genzyme and BMS. JD is a consultant for Blue Earth Diagnostics, Magnolia, Gamaka Bio, and Unum Therapeutics. JD has received research support from Beacon Biosignals, Boehringer Ingelheim, Brystol-Myers Squibb, Eli Lilly, Medimmune, Acerta Pharma, Orbus Therapeutics, and Novartis Pharmaceuticals. JD has received royalties from Wolters Kluwer for serving as an author for UpToDate. MD has research funding from Novartis and Eli Lilly, has served as a consultant for Roche-Genentech, Tillotts Pharma, ORIC Pharmaceuticals, Partner Therapeutics, and Moderna, and is a member of the Scientific Advisory Board for Neoleukin Therapeutics. CTD has served on advisory boards for Argenx and Dysimmune Diseases Foundation. He has received royalties from Oakstone Publishing. He has received grant support from NINDS/NeuroNext. DD has served on an advisory board and/or consulted for UCB, Astellas and Immunovant pharmaceuticals. All compensation for the consulting activities is paid to Mayo Clinic. He has patents pending for KLHL11 and LUZP4 as markers of neurological autoimmunity and germ cell tumors. JG has received research to UCSF support from Genentech/Roche for a clinical trial, performed consulting for Biogen, and received personal compensation for medical-legal consulting. JTG has served as a consultant in past 12 months for Immunovant, Alexion, Momenta, Ra Pharma, Grifols, Jacobus, Cabaletta, Regeneron, Argenx, Signant, UCB, Toleranzia and Piedmont Pharmaceuticals. He receives industry grant support from UCB pharma for a fellowship training grant. Full disclosure statement available at: https://dcri.org/about-us/conflict-of-interest/. DBJ has served on advisory boards for Array Biopharma, BMS, Catalyst Biopharma, Iovance, Jansen, Merck, Novartis, and Oncosec, and has received research funding from BMS and Incyte. VCJ is a site investigator in myasthenia gravis research trials sponsored by PCORI and by Alexion Pharmaceuticals. RK receives research funding from Alexion Pharmaceuticals. NK reports no relevant disclosures. NRL is a consultant and has received honoraria from Bayer, Seattle Genetics, Sanofi, Fortress Biotech, Silverback Therapeutics and SYNOX Therapeutics. JL reports no disclosures. AM reports no disclosures. MM-L reports no relevant disclosures. MJM has served on an advisory board and/or consulted with AstraZeneca Pharmaceuticals, Nektar Therapeutics, Catalyst Pharmaceuticals and Immunai. JN has received research funding from Merck and AstraZeneca; served as a consultant/advisory board member with Merck, AstraZeneca, BMS, Pfizer, Takeda, Roche/Genentech, Daiichi/Sankyo and has received honoraria from Merck, AstraZeneca, BMS, Pfizer, Takeda, Roche/Genentech. TGN reports acting as a consultant for Parexel, Bristol Myers-Squibb, H3 Biomedicine, AbbVie, and Intrinsic Imaging unrelated to the current research. TGN reports grant funding from AstraZeneca unrelated to current research. DR has been an advisor or consultant with AbbVie; Advantagene; Agenus; Agios; Amgen; Bayer; Boston Biomedical; Boehringer Ingelheim; Bristol-Myers Squibb; Celldex; Deciphera; DelMar; EMD Serono; Genenta; Genentech/Roche; Imvax; Inovio; Kintara; Kiyatec; Medicenna Biopharma; Merck; Merck KGaA; Monteris; Neuvogen; Novartis; Novocure; Oncorus; Oxigene; Regeneron; Stemline; Sumitono Dainippon Pharma; Taiho Oncology. Research support to his institution has been provided by Acerta Phamaceuticals; Agenus; Celldex; EMD Serono; Incyte; Inovio; Omniox; Tragara. KMR has served on an advisory board and/or consulted with Merck, BMS, and Eisai. BDS has served on an advisory board and/or consulted with Janssen, Kite/Gilead, and Celgene/BMS. RS has served on an advisory board and/or consulted with AstraZeneca, Bristol-Myers Squib, Eisai, Iovance, Merck, Novartis, Oncosec, Pfizer, and Replimune. He has received research funding from Merck. NW has served on an advisory board with Seattle Genetics, received royalties from Wolters Kluwer and research support from Merck. KW reports no disclosures. LZ has been a consultant for Merck. WCL is an employee of the not-for-profit corporation Project DS, with a trade name of Project Data Sphere. KLR has received personal compensation from Teladoc research support from Project Data Sphere for a irAE-N registry.
Figures
References
-
- Cancer research Institute Timeline of progress. Available: https://www.cancerresearch.org/immunotherapy/timeline-of-progress
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous