

SARS-CoV-2 antibody dynamics and transmission from community-wide serological testing in the Italian municipality of Vo'
- PMID: 34282139
- PMCID: PMC8289856
- DOI: 10.1038/s41467-021-24622-7
SARS-CoV-2 antibody dynamics and transmission from community-wide serological testing in the Italian municipality of Vo'
Erratum in
-
Author Correction: SARS-CoV-2 antibody dynamics and transmission from community-wide serological testing in the Italian municipality of Vo'.Nat Commun. 2021 Aug 12;12(1):5020. doi: 10.1038/s41467-021-25321-z. Nat Commun. 2021. PMID: 34385465 Free PMC article. No abstract available.
Abstract
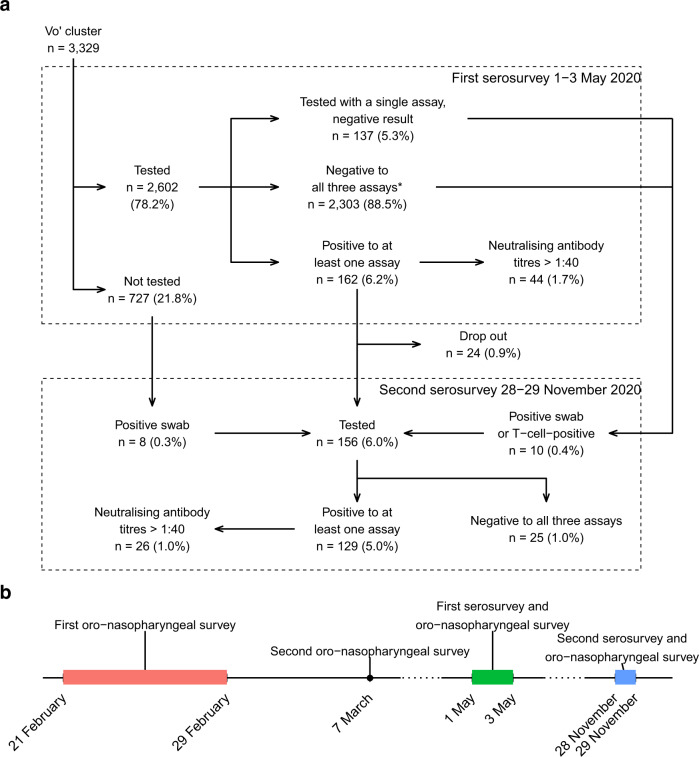
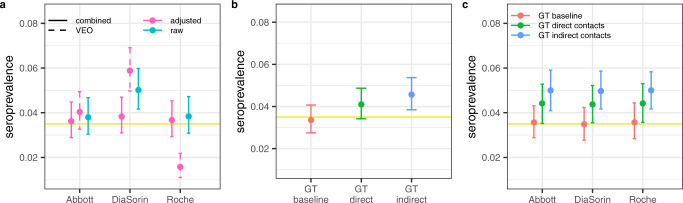
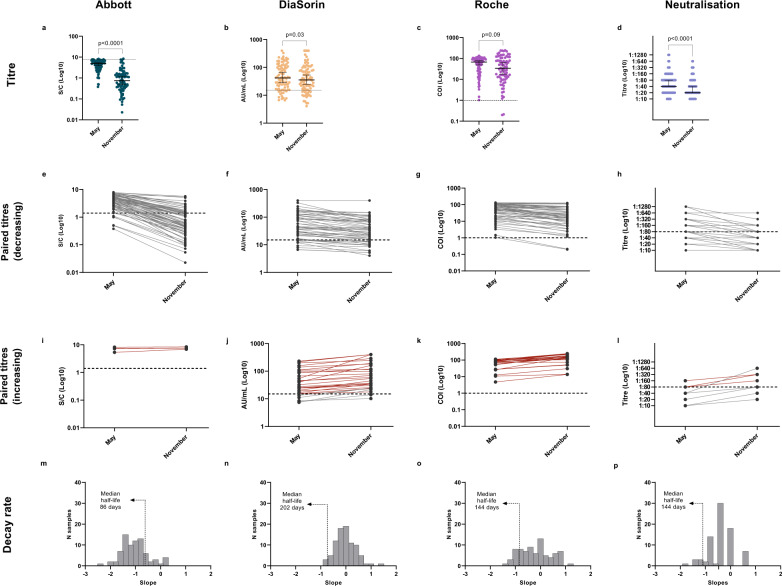
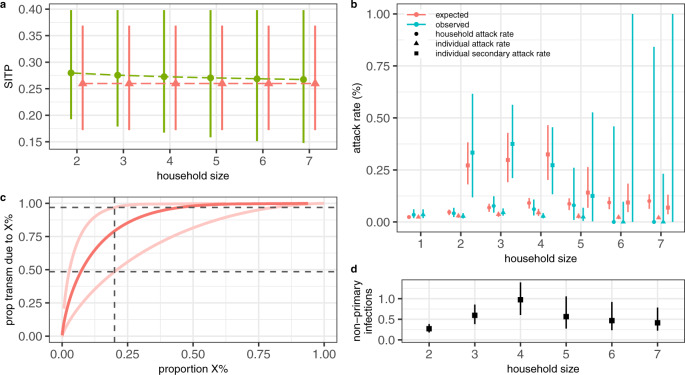
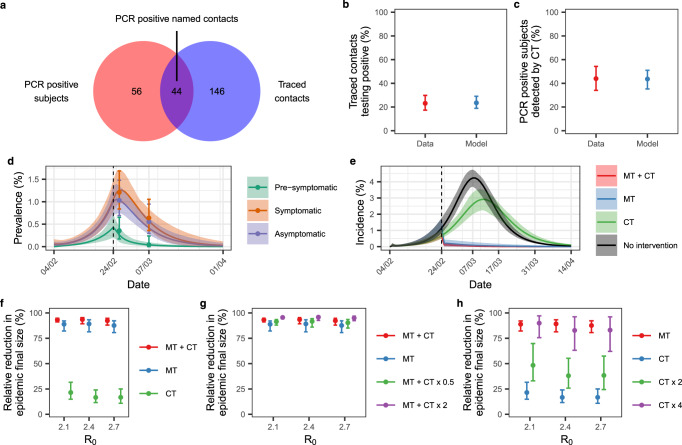
In February and March 2020, two mass swab testing campaigns were conducted in Vo', Italy. In May 2020, we tested 86% of the Vo' population with three immuno-assays detecting antibodies against the spike and nucleocapsid antigens, a neutralisation assay and Polymerase Chain Reaction (PCR). Subjects testing positive to PCR in February/March or a serological assay in May were tested again in November. Here we report on the results of the analysis of the May and November surveys. We estimate a seroprevalence of 3.5% (95% Credible Interval (CrI): 2.8-4.3%) in May. In November, 98.8% (95% Confidence Interval (CI): 93.7-100.0%) of sera which tested positive in May still reacted against at least one antigen; 18.6% (95% CI: 11.0-28.5%) showed an increase of antibody or neutralisation reactivity from May. Analysis of the serostatus of the members of 1,118 households indicates a 26.0% (95% CrI: 17.2-36.9%) Susceptible-Infectious Transmission Probability. Contact tracing had limited impact on epidemic suppression.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- World Health Organization, WHO Coronavirus Disease (COVID-19) Dashboard. Available at https://covid19.who.int/. (Accessed 23 February 2021).
-
- European Centre for Disease Control and Prevention. COVID-19 situation update for the EU/EEA as of week 6, updated 18 February 2021. Available at https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea. (Accessed 23 February 2021).
-
- EpidemicForecasting.org, Epidemic forecasting global NPI database (2020). Available at http://epidemicforecasting.org/datasets. (Accessed 23 February 2021).
-
- Hale, T. et al. Oxford COVID-19 Government Response Tracker, Blavatnik School of Government (2020). Available at www.bsg.ox.ac.uk/research/research-projects/coronavirus-government-respo.... (Accessed 23 February 2021).
-
- European Centres for Disease Control. Data on Country Response measures to COVID-19. Available at https://www.ecdc.europa.eu/en/publications-data/download-data-response-m.... (Accessed 23 February 2021).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
