

Dynamics of inhaled corticosteroid use are associated with asthma attacks
- PMID: 34282212
- PMCID: PMC8289909
- DOI: 10.1038/s41598-021-94219-z
Dynamics of inhaled corticosteroid use are associated with asthma attacks
Abstract
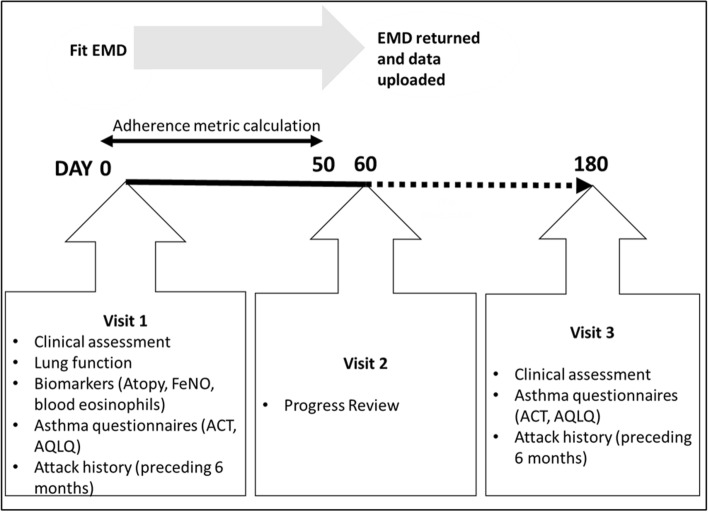
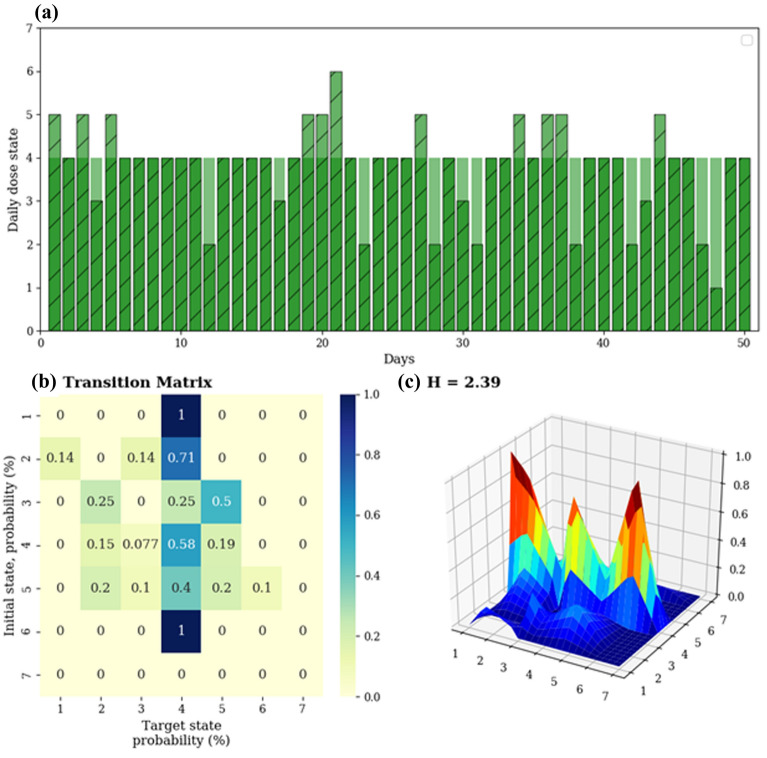
Inhaled corticosteroids (ICS) suppress eosinophilic airway inflammation in asthma, but patients may not adhere to prescribed use. Mean adherence-averaging total doses taken over prescribed-fails to capture many aspects of adherence. Patients with difficult-to-treat asthma underwent electronic monitoring of ICS, with data collected over 50 days. These were used to calculate entropy (H) a measure of irregular inhaler use over this period, defined in terms of transitional probabilities between different levels of adherence, further partitioned into increasing (Hinc) or decreasing (Hdec) adherence. Mean adherence, time between actuations (Gapmax), and cumulative time- and dose-based variability (area-under-the-curve) were measured. Associations between adherence metrics and 6-month asthma status and attacks were assessed. Only H and Hdec were associated with poor baseline status and 6-month outcomes: H and Hdec correlated negatively with baseline quality of life (H:Spearman rS = - 0·330, p = 0·019, Hdec:rS = - 0·385, p = 0·006) and symptom control (H:rS = - 0·288, p = 0·041, Hdec: rS = - 0·351, p = 0·012). H was associated with subsequent asthma attacks requiring hospitalisation (Wilcoxon Z-statistic = - 2.34, p = 0·019), and Hdec with subsequent asthma attacks of other severities. Significant associations were maintained in multivariable analyses, except when adjusted for blood eosinophils. Entropy analysis may provide insight into adherence behavior, and guide assessment and improvement of adherence in uncontrolled asthma.
© 2021. The Author(s).
Conflict of interest statement
MJA holds investigator-initiated grants for unrelated research from Pfizer and Boehringer-Ingelheim. He has undertaken an unrelated consultancy for and received assistance with conference attendance from Sanofi. He has also received a speaker’s fee from GSK. HKR or her institute has received fees for providing independent medical advice on advisory boards for AstraZeneca, GlaxoSmithKline, Boehringer Ingelheim, GlaxoSmithKline, Novartis and Sanofi/Genzyme, for providing independent medical education at symposia funded by AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Mundipharma, Novartis and Teva, and research grants from AstraZeneca, GlaxoSmithKline and Novartis, all unrelated to this research. MH has received grants-in-aid, speaker fees, and fees for serving on the advisory boards of GlaxoSmithKline, AstraZeneca, Novartis, Teva, Sanofi, and Seqirus, all unrelated to the current manuscript, all paid to his institutional employer Alfred Health. JL has received fees for providing unrelated independent medical advice for GlaxoSmithKline and has provided speaker fees for medical education purposes from Boehringer Ingelheim, GlaxoSmithKline and AstraZeneca. HR reports grants and personal fees from AstraZeneca, grants and personal fees from GlaxoSmithKline, personal fees from Merck, grants and personal fees from Novartis, personal fees from Teva, personal fees from Boehringer Ingelheim, personal fees from Sanofi Genzyme, outside the submitted work. CT is a NHMRC Career Development Fellow (Level 1). JL received support through an Australian Government Research Training Program Scholarship. Both funding sources had no role in study design, collection, analysis, interpretation of data, writing of the report of decision to submit this manuscript for publication. JH and JF have no competing interests to disclose.
Figures



References
-
- GINA. Diagnosis and management of difficult-to-treat and severe asthma in adolescent and adult patients. (2019). Available online at https://ginasthma.org/wp-content/uploads/2018/11/GINA-SA-FINAL-wms.pdf.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
