

Congenital ocular counter-roll: a review of cases treated exclusively by ophthalmologists
- PMID: 34282394
- PMCID: PMC8243193
- DOI: 10.18240/ijo.2021.07.17
Congenital ocular counter-roll: a review of cases treated exclusively by ophthalmologists
Abstract
Aim: To review the demographics, clinical manifestations, and surgical experiences of patients with congenital ocular counter-roll, whose treatments were performed exclusively by ophthalmologists.
Methods: A retrospective review was conducted consisting of patients who received strabismus surgery between 2017 to 2019. Patients with obvious ocular counter-roll were included.
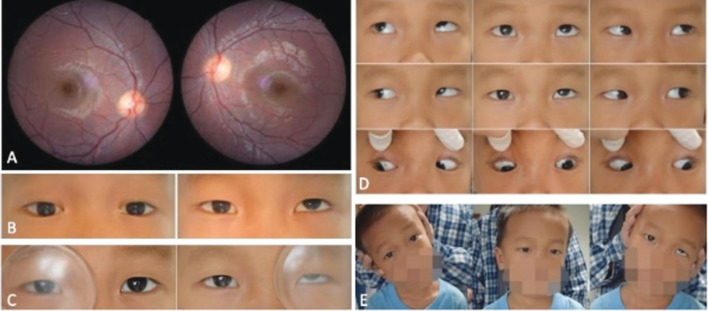
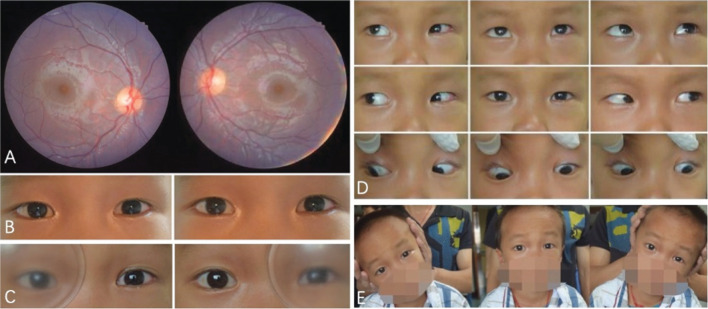
Results: A total of 7008 patients who received strabismus surgery, 28 (12 males, 16 females) were diagnosed as congenital ocular counter-roll, accounting for 0.40%. All patients were initially misdiagnosed: 21 patients were misdiagnosed as superior oblique palsy (SOP), 3 as inferior oblique overaction, 2 as dissociated vertical deviation (DVD), 1 as superior oblique overaction with A-pattern exotropia, and 1 as medial rectus palsy. The mean±SD age was 12.4±9.4y (range 2.5-36y). The most common clinical findings included ocular counter-roll, vertical deviation or vertical deviation combined with outward deviation and head tilt. At follow-up, an excellent surgical result was achieved in 20 patients. Preoperative horizontal deviation of 26±24 prism diopter (PD) and vertical deviation of 18±12 PD were reduced to 0±12 PD (P=0.0001) and 3±4 PD (P=0.001), respectively.
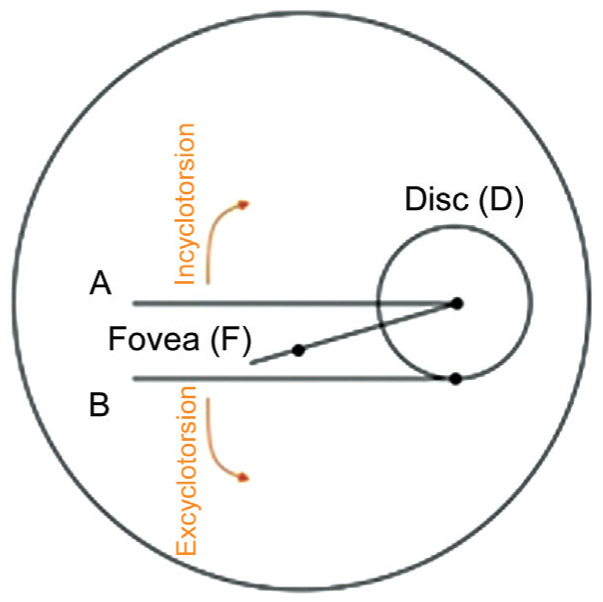
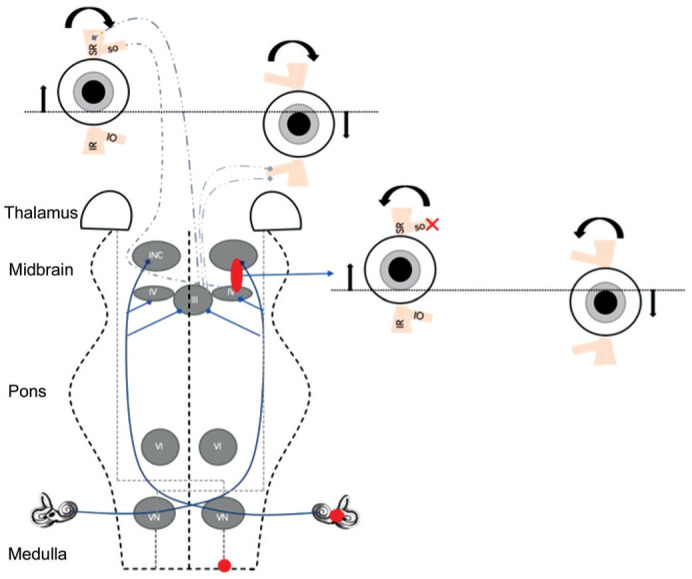
Conclusion: Congenital ocular counter-roll is a rare supranuclear vertical strabismus caused by congenital abnormalities involving vestibule-ocular reflex pathways. In addition to ocular counter-roll, the most salient clinical features included, but are not limited to, hyperdeviation, outward deviation, overelevation in adduction and head tilt.
Keywords: congenital ocular counter-roll; cyclovertical strabismus; skew deviation.
International Journal of Ophthalmology Press.
Figures
Similar articles
-
Surgical management of Helveston syndrome (triad of A- pattern exotropia, superior oblique overaction and dissociated vertical deviation) using 'Four Oblique' procedure.Indian J Ophthalmol. 2020 Jan;68(1):170-173. doi: 10.4103/ijo.IJO_196_19. Indian J Ophthalmol. 2020. PMID: 31856501 Free PMC article.
-
Principles and general strabismus surgical rules in cyclovertical eye muscle palsies.Binocul Vis Strabolog Q Simms Romano. 2012;27(4):249-63. Binocul Vis Strabolog Q Simms Romano. 2012. PMID: 23234487
-
How Lingering Fusional Adaptation Influences the Bielschowsky Head Tilt Test in Superior Oblique Paresis.Klin Monbl Augenheilkd. 2022 Oct;239(10):1213-1220. doi: 10.1055/a-1933-3223. Epub 2022 Oct 18. Klin Monbl Augenheilkd. 2022. PMID: 36257303 English.
-
[Clinical manifestations and treatment of Skew deviation].Zhonghua Yan Ke Za Zhi. 2012 Sep;48(9):856-60. Zhonghua Yan Ke Za Zhi. 2012. PMID: 23141582 Review. Chinese.
-
[Difficulties in diagnosis and treatment of dissociated vertical deviation (DVD). Part I].Klin Oczna. 2007;109(7-9):356-8. Klin Oczna. 2007. PMID: 18260298 Review. Polish.
References
-
- Donahue SP, Itharat P. A-pattern strabismus with overdepression in adduction: a special type of bilateral skew deviation? J AAPOS. 2010;14(1):42–46. - PubMed
-
- Kim DH, Kim H, Lim HT. The influence of ocular sighting dominance on fundus torsion in patients with unilateral congenital superior oblique palsy. Graefes Arch Clin Exp Ophthalmol. 2017;255(12):2473–2479. - PubMed
-
- Choi YY, Lee SY. A case of surgery for congenital superior oblique palsy with intorsion of nonparalized eye. Journal of The Korean Ophthalmological Society. 2003;44(4):1002–1009.
LinkOut - more resources
Full Text Sources