

Hypertensive Retinopathy and the Risk of Stroke Among Hypertensive Adults in China
- PMID: 34283210
- PMCID: PMC8300046
- DOI: 10.1167/iovs.62.9.28
Hypertensive Retinopathy and the Risk of Stroke Among Hypertensive Adults in China
Abstract
Purpose: This study aimed to investigate the association between hypertensive retinopathy and the risk of first stroke, examine possible effect modifiers in hypertensive patients, and test the appropriateness of the Keith-Wagener-Barker (KWB) classification for predicting stroke risk.
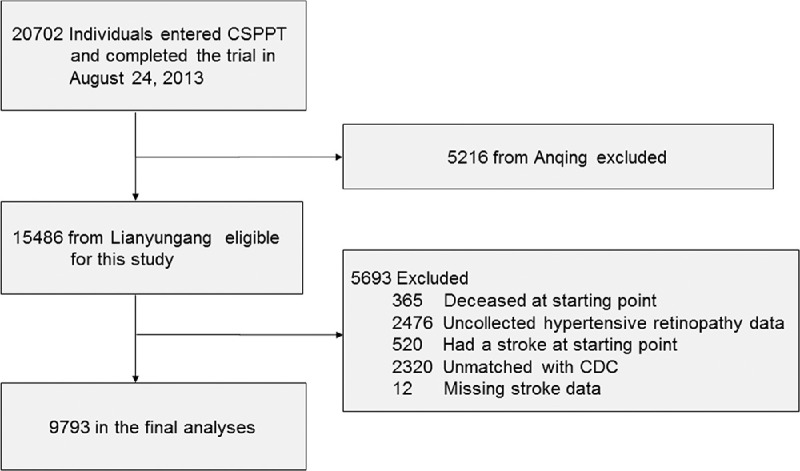
Methods: In total, 9793 hypertensive participants (3727 males and 6066 females) without stroke history from the China Stroke Primary Prevention Trial were included in this study. The primary outcome was first stroke.
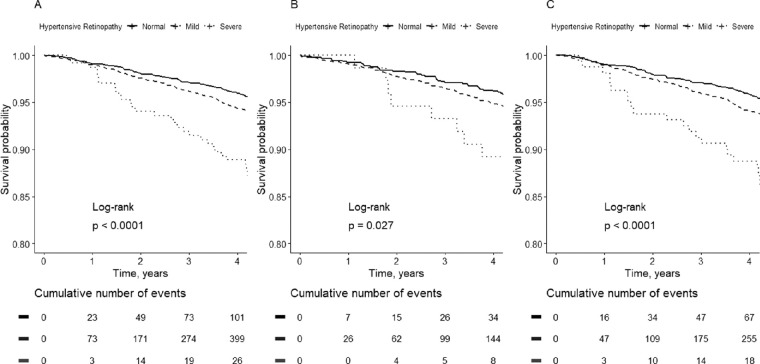
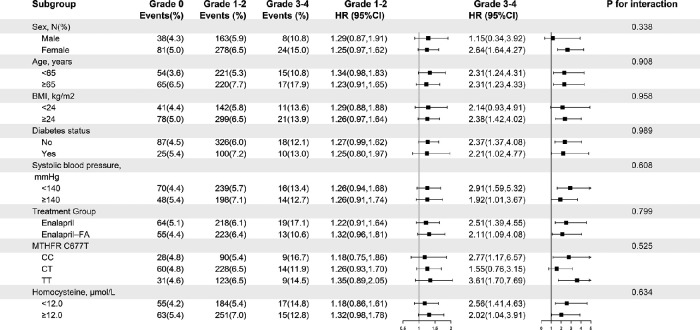
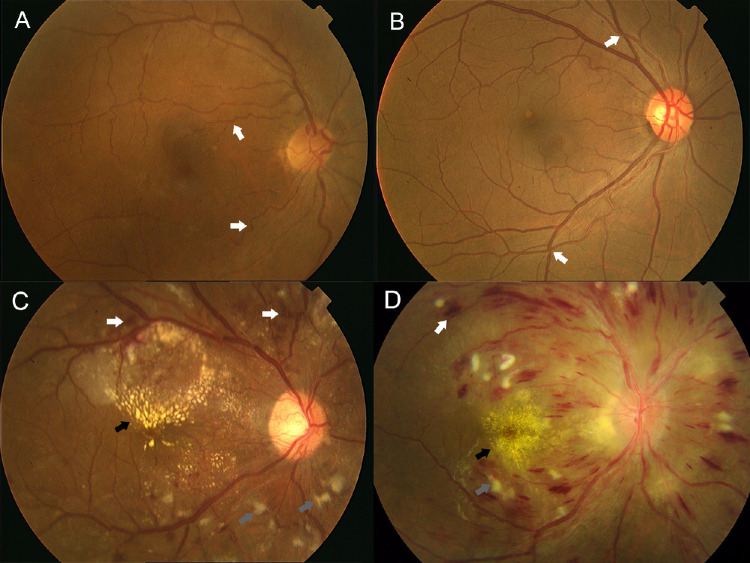
Results: Over a median follow-up of 4.4 years, 592 participants experienced their first stroke (509 ischemic, 77 hemorrhagic, and six unclassifiable strokes). In total, 5590 participants were diagnosed with grade 1 retinopathy (57.08%), 1466 with grade 2 retinopathy (14.97%), 231 with grade 3 retinopathy (2.36%), and three with grade 4 retinopathy (0.03%). Grades 1 and 2 were merged and classified as mild retinopathy, and grades 3 and 4 were merged and classified as severe retinopathy. There was a significant positive association between hypertensive retinopathy and the risk of first stroke and first ischemic stroke, and no effect modifiers were found. The hazard ratios (HRs) for first stroke were as follows: mild versus no retinopathy, 1.26 (95% confidence interval [CI], 1.01-1.58, P = 0.040), and severe versus no retinopathy, 2.40 (95% CI, 1.49-3.84, P < 0.001). The HRs for ischemic stroke were as follows: severe versus no retinopathy, 2.35 (95% CI, 1.41-3.90, P = 0.001), and nonsignificantly increased HRs for mild versus no retinopathy, 1.26 (95% CI, 0.99-1.60, P = 0.057).
Conclusions: There was a significant positive association between hypertensive retinopathy and the risk of first stroke in patients with hypertension, indicating that hypertensive retinopathy may be a predictor of the risk of stroke. A simplified two-grade classification system based on the KWB classification is recommended for predicting stroke risk.
Conflict of interest statement
Disclosure:
Figures
References
-
- Wang W, Jiang B, Sun H, et al.. Prevalence, Incidence, and Mortality of Stroke in China: results from a nationwide population-based survey of 480 687 adults. Circulation. 2017; 135: 759–771. - PubMed
-
- Collins R, Peto R, MacMahon S, et al.. Blood pressure, stroke, and coronary heart disease. Part 2, Short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet. 1990; 335: 827–838. - PubMed
-
- MacMahon S, Peto R, Cutler J, et al.. Blood pressure, stroke, and coronary heart disease. Part 1, Prolonged differences in blood pressure: Prospective observational studies corrected for the regression dilution bias. Lancet. 1990; 335: 765–774. - PubMed
-
- Powers WJ, Zazulia AR.. The use of positron emission tomography in cerebrovascular disease. Neuroimaging Clin N Am. 2003; 13: 741–758. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
