

A breakthrough series collaborative to increase patient participation with hemodialysis tasks: A stepped wedge cluster randomised controlled trial
- PMID: 34283851
- PMCID: PMC8291659
- DOI: 10.1371/journal.pone.0253966
A breakthrough series collaborative to increase patient participation with hemodialysis tasks: A stepped wedge cluster randomised controlled trial
Abstract
Background: Compared to in-centre, home hemodialysis is associated with superior outcomes. The impact on patient experience and clinical outcomes of consistently providing the choice and training to undertake hemodialysis-related treatment tasks in the in-centre setting is unknown.
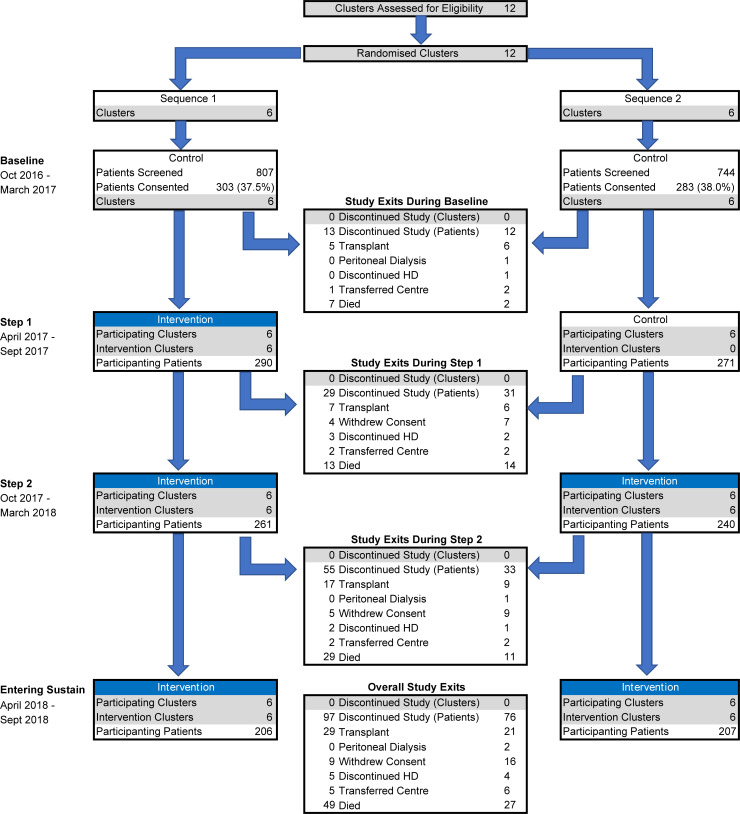
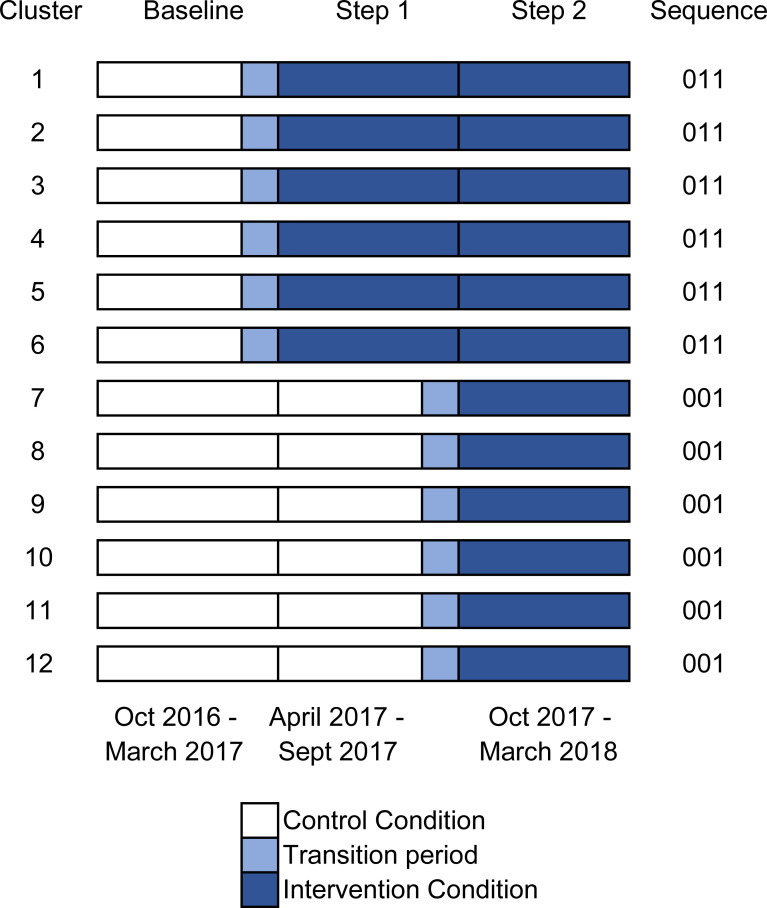
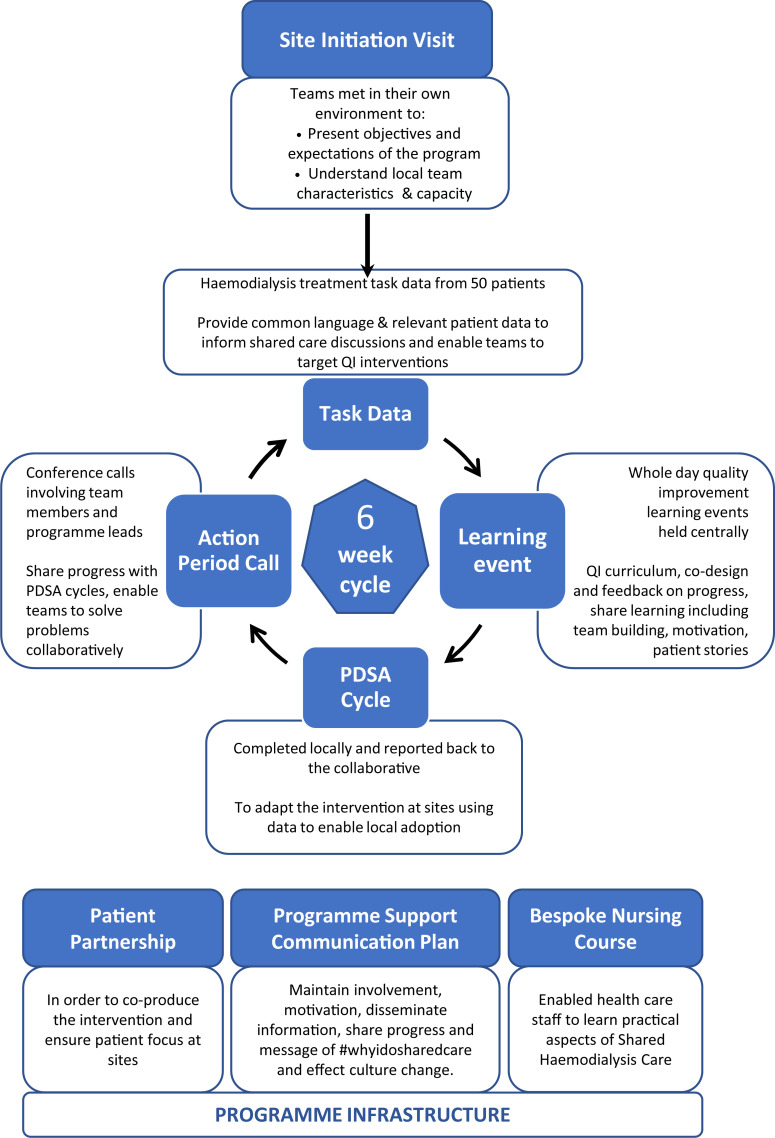
Methods: A stepped-wedge cluster randomised trial in 12 UK renal centres recruited prevalent in-centre hemodialysis patients with sites randomised into early and late participation in a 12-month breakthrough series collaborative that included data collection, learning events, Plan-Study-Do-Act cycles, and teleconferences repeated every 6 weeks, underpinned by a faculty, co-production, materials and a nursing course. The primary outcome was the proportion of patients undertaking five or more hemodialysis-related tasks or home hemodialysis. Secondary outcomes included independent hemodialysis, quality of life, symptoms, patient activation and hospitalisation. ISRCTN Registration Number 93999549.
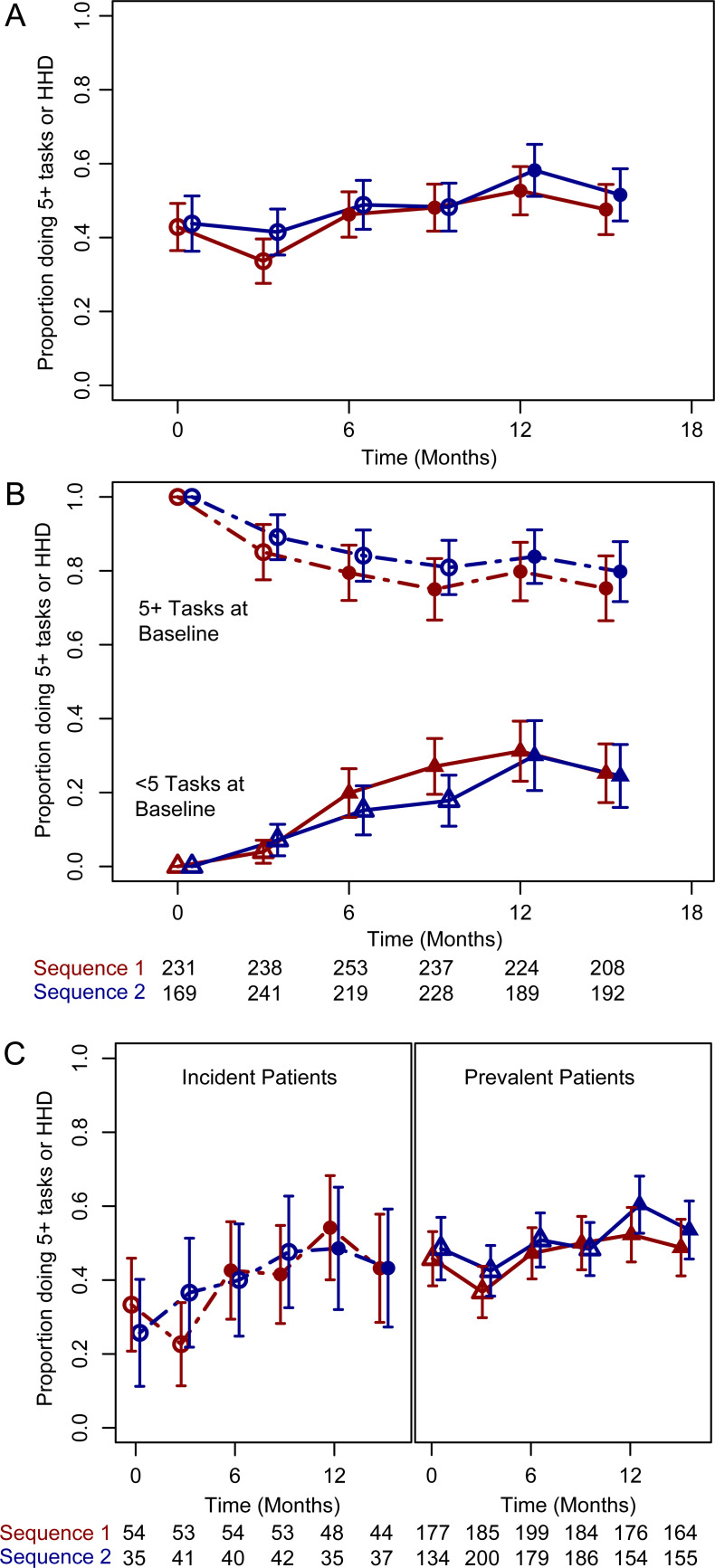
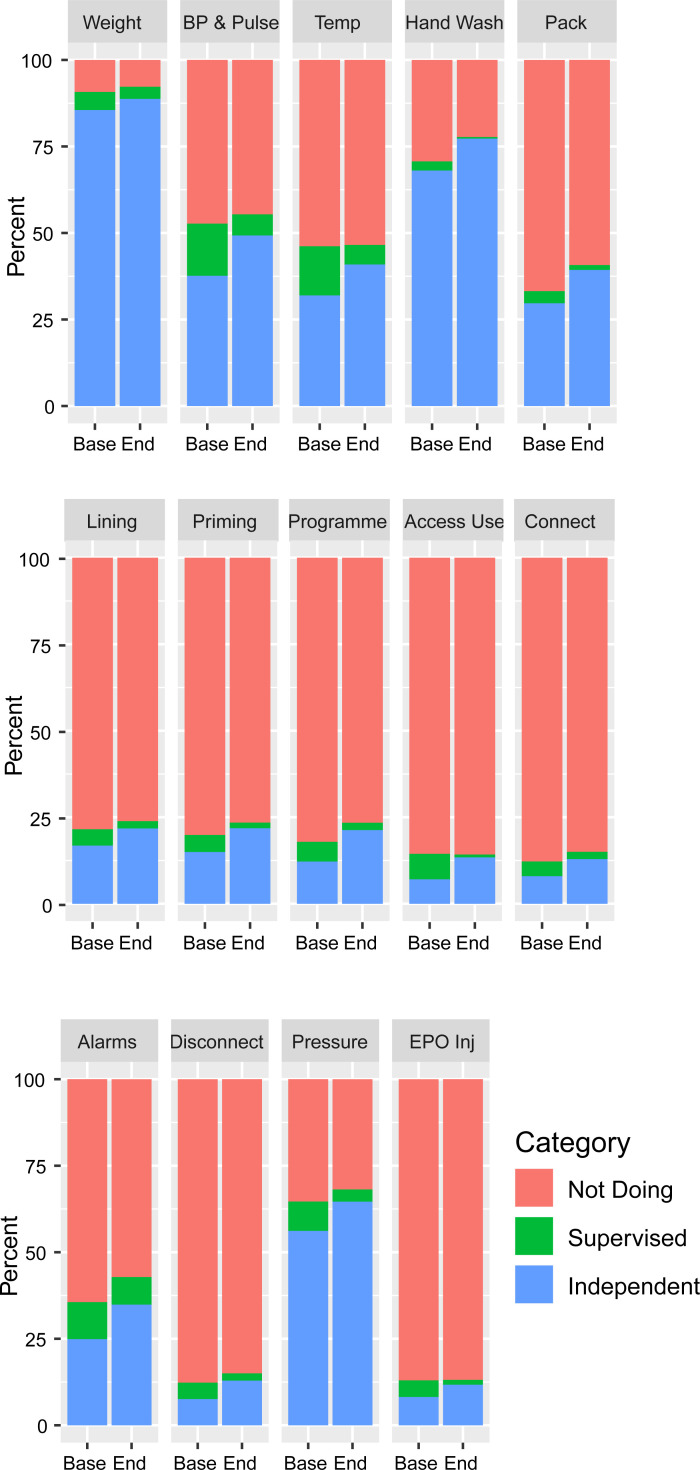
Results: 586 hemodialysis patients were recruited. The proportion performing 5 or more tasks or home hemodialysis increased from 45.6% to 52.3% (205 to 244/449, difference 6.2%, 95% CI 1.4 to 11%), however after analysis by step the adjusted odds ratio for the intervention was 1.63 (95% CI 0.94 to 2.81, P = 0.08). 28.3% of patients doing less than 5 tasks at baseline performed 5 or more at the end of the study (69/244, 95% CI 22.2-34.3%, adjusted odds ratio 3.71, 95% CI 1.66-8.31). Independent or home hemodialysis increased from 7.5% to 11.6% (32 to 49/423, difference 4.0%, 95% CI 1.0-7.0), but the remaining secondary endpoints were unaffected.
Conclusions: Our intervention did not increase dialysis related tasks being performed by a prevalent population of centre based patients, but there was an increase in home hemodialysis as well as an increase in tasks among patients who were doing fewer than 5 at baseline. Further studies are required that examine interventions to engage people who dialyse at centres in their own care.
Conflict of interest statement
JF has received speaker honoraria from Fresenius medical care and Novartis, and conducts research funded by the National Institute of Health Research (NIHR), Vifor Pharma and Novartis. MEW has received speaker honoraria Fresenius and Baxter, has acted on an advisory board for Baxter and has conducted research funded by the NIHR. SJW has received book royalties from Wiley and has received funds from NIHR, the Department of Health and Medical Research Council. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Saran R, Robinson B, Abbott KC, Agodoa LY, Albertus P, Ayanian J, et al.. US Renal Data System 2016 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am J Kidney Dis. 2017;69(3 Suppl 1):A7–A8. Epub 2017/02/27. doi: 10.1053/j.ajkd.2016.12.004 ; PubMed Central PMCID: PMC6605045. - DOI - PMC - PubMed
-
- Gair R, Steenkamp M. Valuing Individuals: Transforming Participation in Chronic Kidney Disease2016. Available from: https://www.thinkkidneys.nhs.uk/ckd/resources/reports/.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
