

US Database Study of Clinical Burden and Unmet Need in Recurrent Pericarditis
- PMID: 34284595
- PMCID: PMC8475691
- DOI: 10.1161/JAHA.120.018950
US Database Study of Clinical Burden and Unmet Need in Recurrent Pericarditis
Abstract
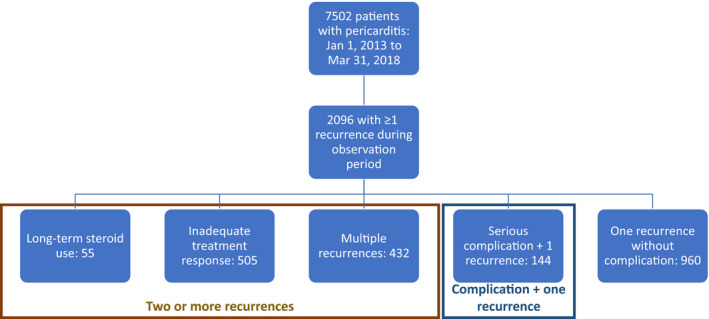
Background Patients with recurrent pericarditis (RP) may develop complications, multiple recurrences, or inadequate treatment response. This study aimed to characterize disease burden and unmet needs in RP. Methods and Results This retrospective US database analysis included newly diagnosed patients with RP with ≥24 months of continuous history following their first pericarditis episode. RP was defined as ≥2 pericarditis episodes ≥28 days apart. Some patients had ≥2 recurrences, while others had a single recurrence with a serious complication, ie, constrictive pericarditis, cardiac tamponade, or a large pericardial effusion with pericardiocentesis/pericardial window. Among these patients with multiple recurrences and/or complications, some had features relating to treatment history, including long-term corticosteroid use (corticosteroids started within 30 days of flare, continuing ≥90 consecutive days) or inadequate treatment response (pericarditis recurring despite corticosteroids and/or colchicine, or other drugs [excluding NSAIDs] within 30 days of flare, or prior pericardiectomy). Patients (N=2096) had hypertension (60%), cardiomegaly (9%), congestive heart failure (17%), atrial fibrillation (16%), autoimmune diseases (18%), diabetes mellitus (21%), renal disease (20%), anxiety (21%), and depression (14%). Complications included pericardial effusion (50%), cardiac tamponade (9%), and constrictive pericarditis (4%). Pharmacotherapy included colchicine (51%), NSAIDs (40%), and corticosteroids (30%), often in combination. This study estimates 37 000 US patients with RP; incidence was 6.0/100 000/year (95% CI, 5.6‒6.3), and prevalence was 11.2/100 000 (95% CI, 10.6‒11.7). Conclusions Patients with RP may have multiple recurrences and/or complications, often because of inadequate treatment response and persistent underlying disease. Corticosteroid use is frequent despite known side-effect risks, potentially exacerbated by prevalent comorbidities. Substantial clinical burden and lack of effective treatments underscore the high unmet need.
Keywords: database analysis; epidemiology; pericarditis; recurrent pericarditis.
Conflict of interest statement
Allan Klein received research grants from Kiniksa Corporation and served as an advisory board member for Kiniksa and Sobi. Paul Cremer served as an advisory board member for Sobi. Apostolos Kontzias served as a consultant for Novartis, Horizon, Sobi, and Kiniksa. Ryan Tubman and Mike Roy are employees of Clearview Health Partners. Matthew Magestro and Michelle Lim‐Watson are employees of Kiniksa Pharmaceuticals Corporation. Muhammad Furqan has no disclosures to report.
Figures
References
-
- Adler Y, Charron P, Imazio M, Badano L, Barón‐Esquivias G, Bogaert J, Brucato A, Gueret P, Klingel K, Lionis C, et al. 2015 ESC guidelines for the diagnosis and management of pericardial diseases: the Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC) endorsed by: the European Association for Cardio‐Thoracic Surgery (EACTS). Eur Heart J. 2015;36:2921–2964. DOI: 10.1093/eurheartj/ehv318. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
