

The effect of leisure time physical activity and sedentary behaviour on the health of workers with different occupational physical activity demands: a systematic review
- PMID: 34284795
- PMCID: PMC8290554
- DOI: 10.1186/s12966-021-01166-z
The effect of leisure time physical activity and sedentary behaviour on the health of workers with different occupational physical activity demands: a systematic review
Abstract
Background: Although it is generally accepted that physical activity reduces the risk for chronic non-communicable disease and mortality, accumulating evidence suggests that occupational physical activity (OPA) may not confer the same health benefits as leisure time physical activity (LTPA). It is also unclear if workers in high OPA jobs benefit from LTPA the same way as those in sedentary jobs. Our objective was to determine whether LTPA and leisure time sedentary behaviour (LTSB) confer the same health effects across occupations with different levels of OPA.
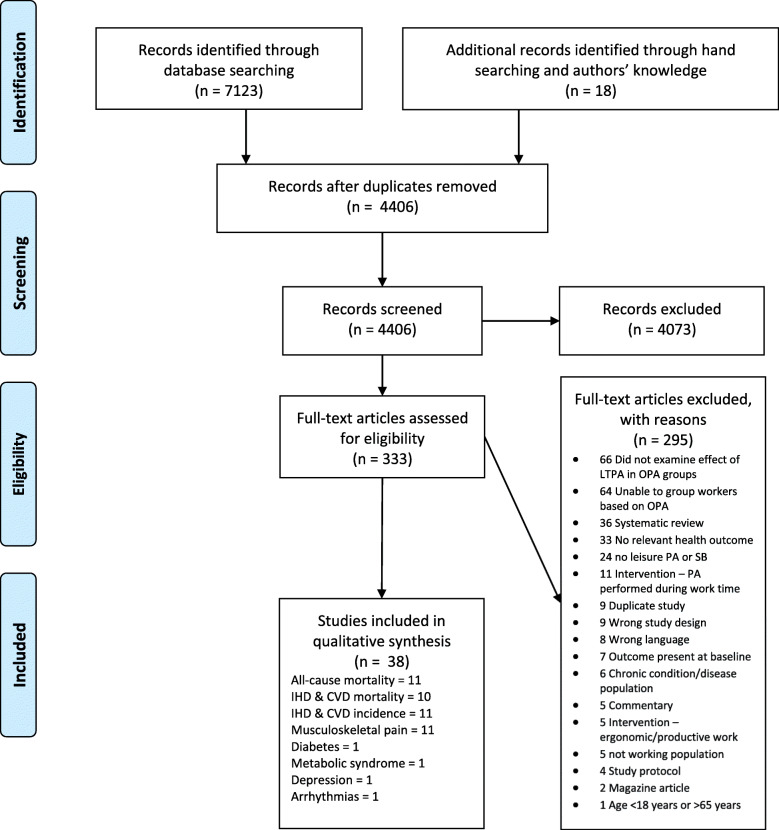
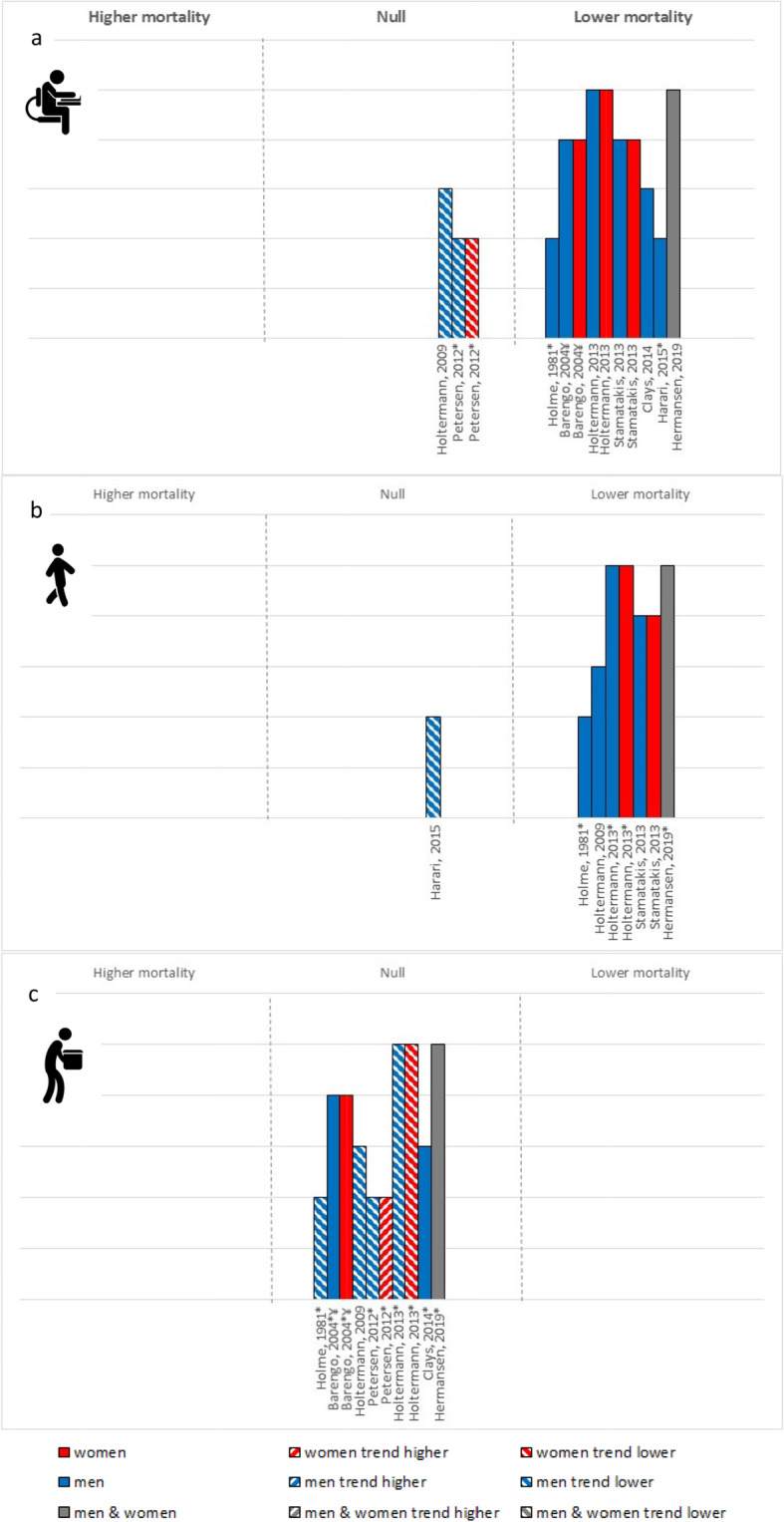
Methods: Searches were run in Medline, Embase, PsycINFO, ProQuest Public Health and Scopus from inception to June 9, 2020. Prospective or experimental studies which examined the effects of LTPA or LTSB on all-cause and cardiovascular mortality and cardiovascular disease, musculoskeletal pain, diabetes, metabolic syndrome, arrhythmias and depression among adult workers grouped by OPA (low OPA/sitters, standers, moderate OPA/intermittent movers, high OPA/heavy labourers) were eligible. Results were synthesized using narrative syntheses and harvest plots, and certainty of evidence assessed with GRADE.
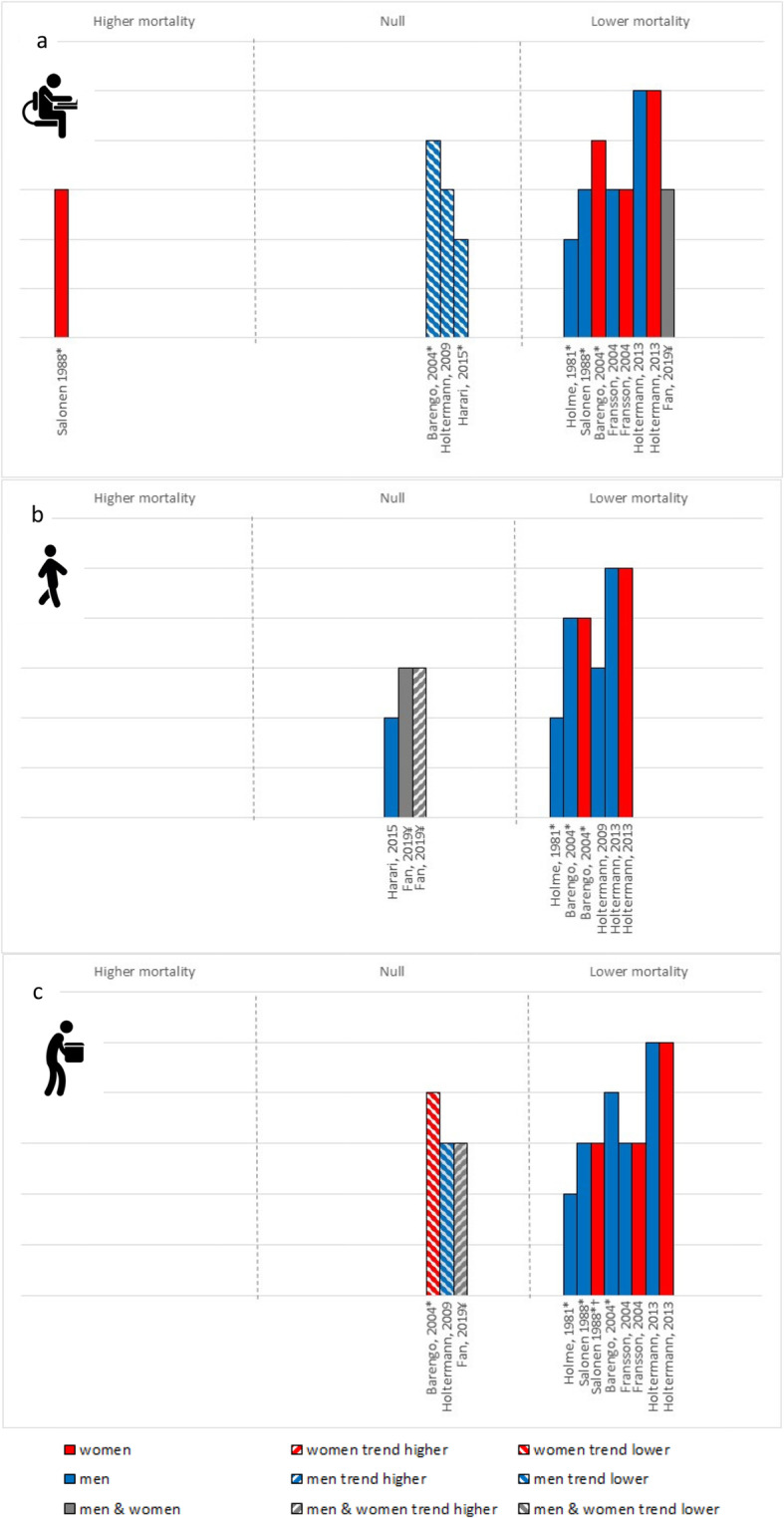
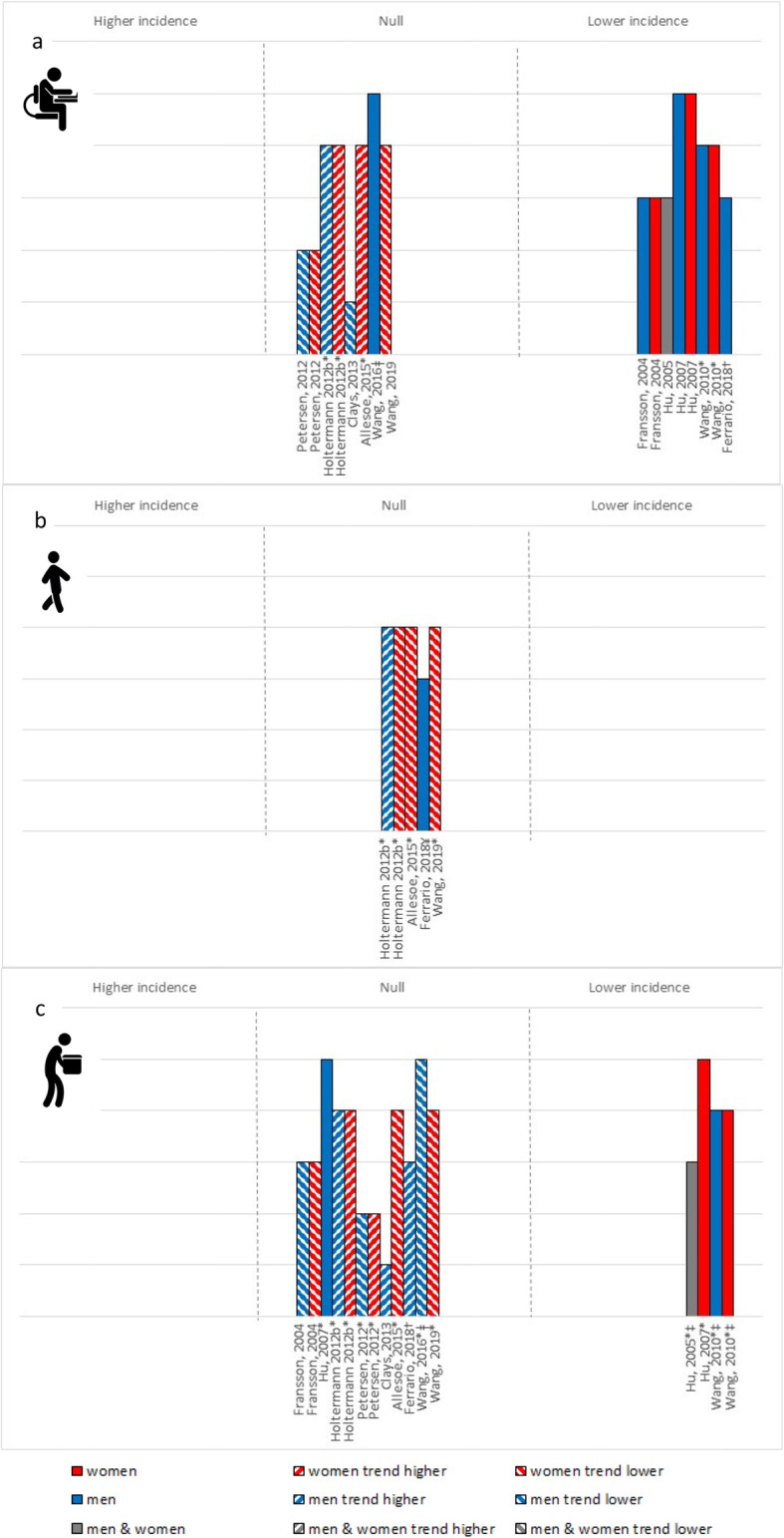
Results: The review includes 38 papers. Across all outcomes, except cardiovascular mortality, metabolic syndrome and atrial fibrillation, greater LTPA was consistently protective among low OPA, but conferred less protection among moderate and high OPA. For cardiovascular mortality and metabolic syndrome, higher levels of LTPA were generally associated with similar risk reductions among all OPA groups. Few studies examined effects in standers and none examined effects of LTSB across OPA groups.
Conclusions: Evidence suggests that LTPA is beneficial for all workers, but with larger risk reductions among those with low compared to high OPA jobs. This suggests that, in our attempts to improve the health of workers through LTPA, tailored interventions for different occupational groups may be required. More high-quality studies are needed to establish recommended levels of LTPA/LTSB for different OPA groups.
Protocol registration: PROSPERO # CRD42020191708 .
Keywords: Cardiovascular disease; Leisure; Mortality; Occupation; Physical activity; Sedentary behaviour.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Saunders TJ, McIsaac T, Douillette K, Gaulton N, Hunter S, Rhodes RE, Prince SA, Carson V, Chaput JP, Chastin S, Giangregorio L, Janssen I, Katzmarzyk PT, Kho ME, Poitras VJ, Powell KE, Ross R, Ross-White A, Tremblay MS, Healy GN. Sedentary behaviour and health in adults: an overview of systematic reviews. Appl Physiol Nutr Metab. 2020;45(10):S197–S217. doi: 10.1139/apnm-2020-0272. - DOI - PubMed
-
- 2018 Physical Activity Guidelines Advisory Committee . 2018 physical activity guidelines advisory committee scientific report. Washington, DC, US: Department of Health and Human Services; 2018.
-
- Holtermann A, Krause N, van der Beek AJ, Straker L. The physical activity paradox: six reasons why occupational physical activity (OPA) does not confer the cardiovascular health benefits that leisure time physical activity does. Br J Sports Med. 2018;52(3):149–150. doi: 10.1136/bjsports-2017-097965. - DOI - PubMed
-
- Andersen LL, Fallentin N, Thorsen SV, Holtermann A. Physical workload and risk of long-term sickness absence in the general working population and among blue-collar workers: prospective cohort study with register follow-up. Occup Environ Med. 2016;73(4):246–253. doi: 10.1136/oemed-2015-103314. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
