

Reporting of adverse events, conflict of interest and funding in randomised controlled trials of antibiotics: a secondary analysis
- PMID: 34285004
- PMCID: PMC8292799
- DOI: 10.1136/bmjopen-2020-045406
Reporting of adverse events, conflict of interest and funding in randomised controlled trials of antibiotics: a secondary analysis
Abstract
Objectives: Transparent reporting of trials is necessary to assess their internal and external validity. Currently, little is known about the quality of reporting in antibiotics trials. Our study investigates the reporting of adverse events, conflicts of interest and funding information in trials of penicillins, cephalosporins and macrolides.
Design: A secondary analysis of trials included in a convenience sample of three systematic reviews.
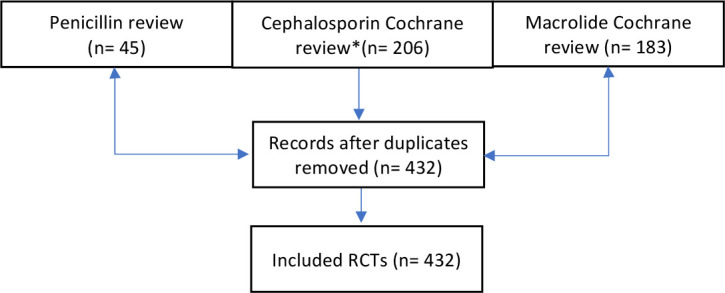
Methods: All randomised controlled trials included in the systematic reviews were included, although duplicates were removed. Eligible trials compared the specified antibiotics to placebo, for any indication. Author pairs independently extracted the data on reporting of adverse events from parent reviews, and data on funding and conflict of interest information from the trial reports. We calculated the overall proportion of trials reporting adverse events, conflict of interest information and funding information, and their proportion before and after the publication of the Consolidated Standards of Reporting Trials (CONSORT) 2001 Statement.
Results: We included 432 trials. Overall, 62% of trials reported adverse events of any kind, although reporting of deaths or antibiotic resistance was less frequent (20% and 37%, respectively). Conflict-of-interest information was provided in 26% of the trials, and funding information was provided in 66% of the trials. There was no significant difference in reporting of adverse events before and after the publication of CONSORT 2001 Statement (62% vs 62%, p=0.92). Conflict of interest statements were provided more frequently (2% vs 55%, p<0.001) and conflict was present more often (0% vs 14%, p<0.001). There was no difference in the provision of the information about trial funding before (62%) and after (70%) CONSORT 2001 publication.
Conclusions: Information about adverse events, conflict of interest and funding, remains under-reported in trials of antibiotics.
Keywords: adverse events; primary care; public health.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Reporting funding source or conflict of interest in abstracts of randomized controlled trials, no evidence of a large impact on general practitioners' confidence in conclusions, a three-arm randomized controlled trial.BMC Med. 2014 Apr 28;12:69. doi: 10.1186/1741-7015-12-69. BMC Med. 2014. PMID: 24779384 Free PMC article. Clinical Trial.
-
Interventions for bacterial folliculitis and boils (furuncles and carbuncles).Cochrane Database Syst Rev. 2021 Feb 26;2(2):CD013099. doi: 10.1002/14651858.CD013099.pub2. Cochrane Database Syst Rev. 2021. PMID: 33634465 Free PMC article.
-
Quality of reporting for pilot randomized controlled trials in the pediatric urology literature-A systematic review.J Pediatr Urol. 2021 Dec;17(6):846-854. doi: 10.1016/j.jpurol.2021.09.012. Epub 2021 Sep 24. J Pediatr Urol. 2021. PMID: 34635440
-
Reporting of drug trial funding sources and author financial conflicts of interest in Cochrane and non-Cochrane meta-analyses: a cross-sectional study.BMJ Open. 2020 May 11;10(5):e035633. doi: 10.1136/bmjopen-2019-035633. BMJ Open. 2020. PMID: 32398334 Free PMC article.
-
Reporting of conflicts of interest from drug trials in Cochrane reviews: cross sectional study.BMJ. 2012 Aug 16;345:e5155. doi: 10.1136/bmj.e5155. BMJ. 2012. PMID: 22906823 Free PMC article.
Cited by
-
The 2021 Dutch Working Party on Antibiotic Policy (SWAB) guidelines for empirical antibacterial therapy of sepsis in adults.BMC Infect Dis. 2022 Aug 11;22(1):687. doi: 10.1186/s12879-022-07653-3. BMC Infect Dis. 2022. PMID: 35953772 Free PMC article.
-
Predictive Factors for Adverse Event Outcomes After Transarterial Radioembolization with Yttrium-90 Resin Microspheres in Europe: Results from the Prospective Observational CIRT Study.Cardiovasc Intervent Radiol. 2023 Jul;46(7):852-867. doi: 10.1007/s00270-023-03391-4. Epub 2023 Mar 13. Cardiovasc Intervent Radiol. 2023. PMID: 36914788 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical