Genomic context of NTRK1/2/3 fusion-positive tumours from a large real-world population
- PMID: 34285332
- PMCID: PMC8292342
- DOI: 10.1038/s41698-021-00206-y
Genomic context of NTRK1/2/3 fusion-positive tumours from a large real-world population
Erratum in
-
Author Correction: Genomic context of NTRK1/2/3 fusion-positive tumours from a large real-world population.NPJ Precis Oncol. 2021 Sep 17;5(1):86. doi: 10.1038/s41698-021-00222-y. NPJ Precis Oncol. 2021. PMID: 34535754 Free PMC article. No abstract available.
Abstract
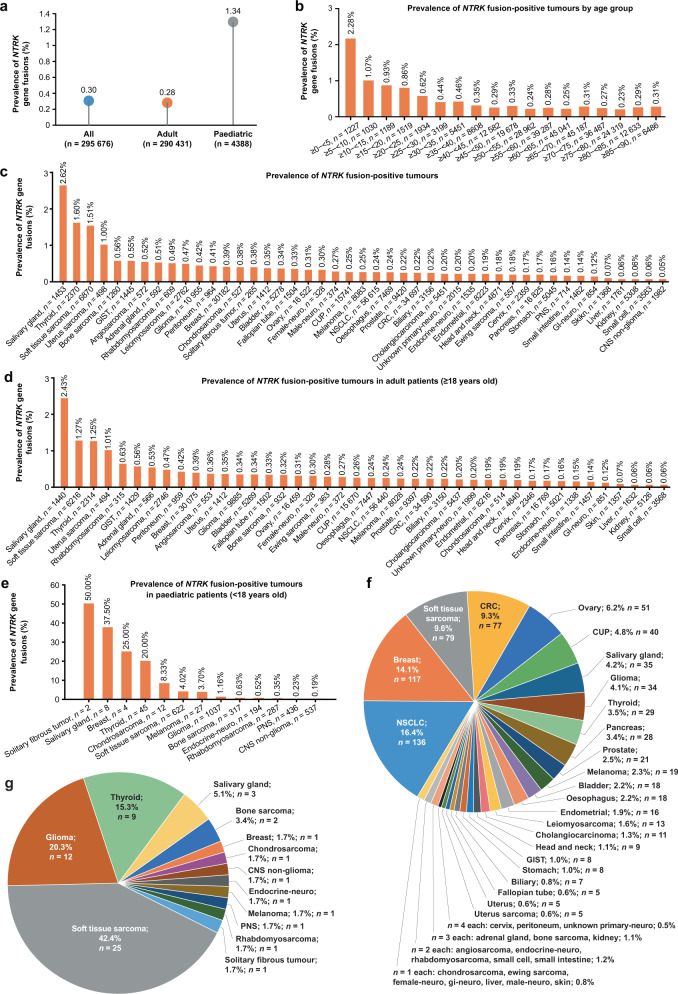
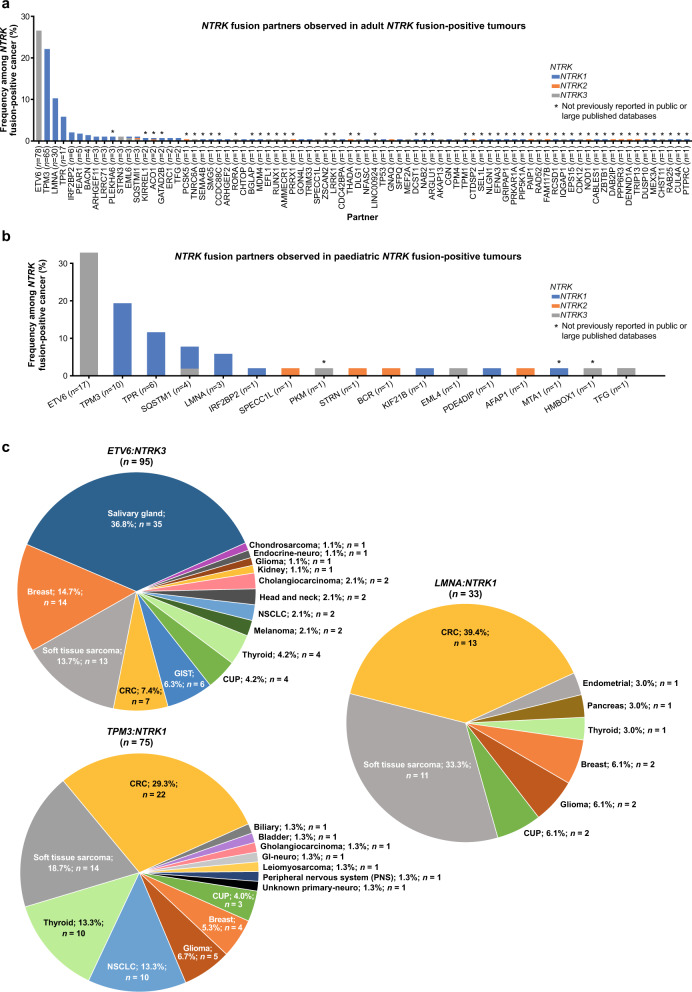
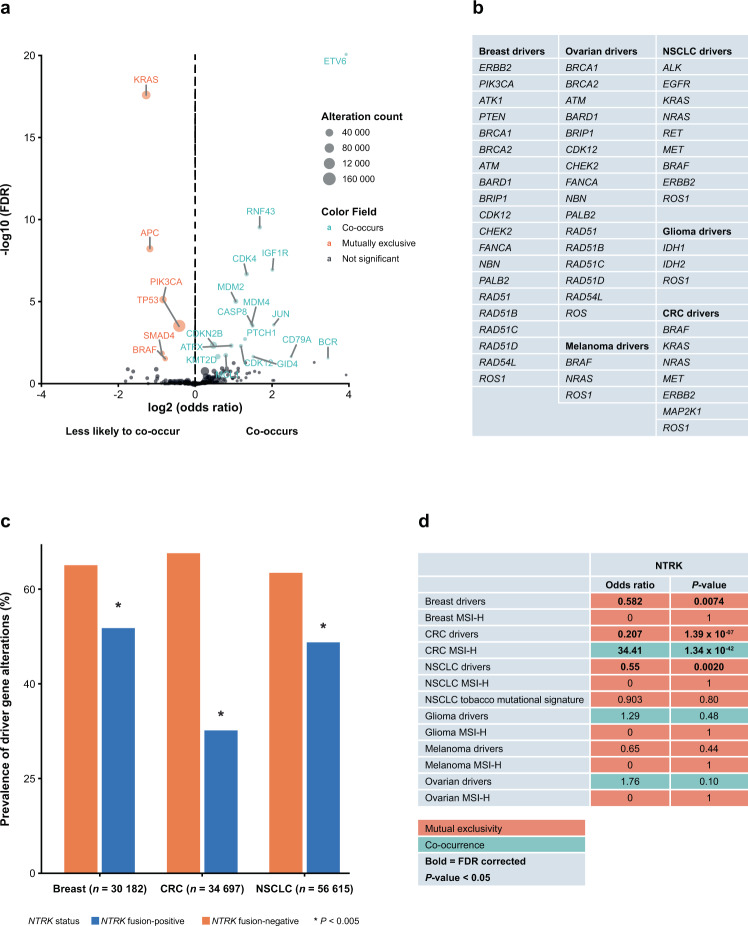
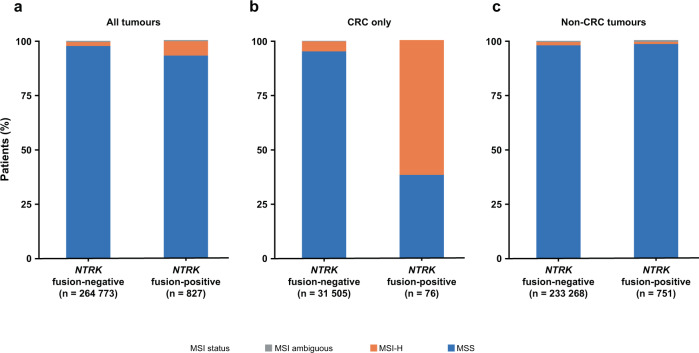
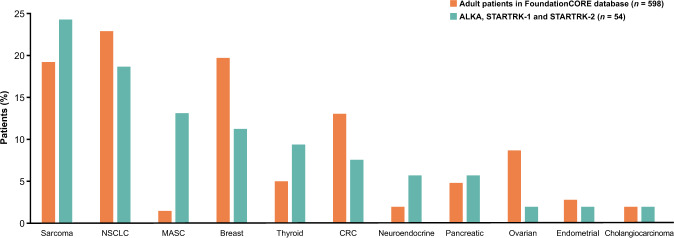
Neurotrophic tropomyosin receptor kinase (NTRK) gene fusions are rare oncogenic drivers in solid tumours. This study aimed to interrogate a large real-world database of comprehensive genomic profiling data to describe the genomic landscape and prevalence of NTRK gene fusions. NTRK fusion-positive tumours were identified from the FoundationCORE® database of >295,000 cancer patients. We investigated the prevalence and concomitant genomic landscape of NTRK fusions, predicted patient ancestry and compared the FoundationCORE cohort with entrectinib clinical trial cohorts (ALKA-372-001 [EudraCT 2012-000148-88]; STARTRK-1 [NCT02097810]; STARTRK-2 [NCT02568267]). Overall NTRK fusion-positive tumour prevalence was 0.30% among 45 cancers with 88 unique fusion partner pairs, of which 66% were previously unreported. Across all cases, prevalence was 0.28% and 1.34% in patients aged ≥18 and <18 years, respectively; prevalence was highest in patients <5 years (2.28%). The highest prevalence of NTRK fusions was observed in salivary gland tumours (2.62%). Presence of NTRK gene fusions did not correlate with other clinically actionable biomarkers; there was no co-occurrence with known oncogenic drivers in breast, or colorectal cancer (CRC). However, in CRC, NTRK fusion-positivity was associated with spontaneous microsatellite instability (MSI); in this MSI CRC subset, mutual exclusivity with BRAF mutations was observed. NTRK fusion-positive tumour types had similar frequencies in FoundationCORE and entrectinib clinical trials. NTRK gene fusion prevalence varied greatly by age, cancer type and histology. Interrogating large datasets drives better understanding of the characteristics of very rare molecular subgroups of cancer and allows identification of genomic patterns and previously unreported fusion partners not evident in smaller datasets.
© 2021. The Author(s).
Conflict of interest statement
C.B.W. has received honoraria from Bayer, Celgene, Ipsen, Medscape, Roche, Servier; participated in advisory boards from Celgene, Shire/Baxalta, Rafael Pharmaceuticals, RedHill, Roche; received travel support from Bayer, Celgene, RedHill, Roche, Servier and Taiho; and received research support from Roche. M.K. has participated in advisory boards from Achilles Therapeutics, Bayer, Janssen, Octimet, OM Pharma and Roche; undertaken consultancy for Roche; received travel grants from AstraZeneca, BerGenBio and Immutep; and received research grants from BerGenBio and Roche. C.L.T. has participated in advisory boards from MSD, BMS, Merck Serono, Roche, Celgene, GSK, Rakuten, Nanobiotix, AstraZeneca and Seattle Genetics. E.S.S., D.X.J., J.Y.N. and D.F. are employees of Foundation Medicine and stockholders in Roche. S.L.M. and T.R.W. are employed by Genentech, Inc. and have equity in Roche. L.V. and M.T. are employed by Roche. F.d.B. reports advisory/consultancy fees from Bristol-Myers Squibb, Eli Lilly, Roche, Amgen, AstraZeneca, Istituto Gentili, Fondazione Internazionale Menarini, Octomet Oncology, Novartis, Merck Sharp & Dohme, Ignyta, Bayer, Noema, ACCMED, Dephaforum, Nadirex, Biotechspert, Pfizer, Tiziana Life Sciences and Pierre Fabre; has participated in speaker bureaus for Bristol-Myers Squibb, Roche, Merck Sharp & Dohme, Ignyta, Dephaforum, prIME Oncology, Pfizer and Biotechespert; has received research grants from Roche, Novartis, Merck Sharp & Dohme, Bristol-Myers Squibb, Pfizer, Kymab, Celgene and Tesaro and travel/accommodation expenses from Bristol-Myers Squibb, Roche, Celgene and Amgen.
Figures