

Comprehensive Mechanism, Novel Markers and Multidisciplinary Treatment of Severe Acute Pancreatitis-Associated Cardiac Injury - A Narrative Review
- PMID: 34285540
- PMCID: PMC8286248
- DOI: 10.2147/JIR.S310990
Comprehensive Mechanism, Novel Markers and Multidisciplinary Treatment of Severe Acute Pancreatitis-Associated Cardiac Injury - A Narrative Review
Erratum in
-
Erratum: Comprehensive Mechanism, Novel Markers and Multidisciplinary Treatment of Severe Acute Pancreatitis-Associated Cardiac Injury - A Narrative Review [Corrigendum].J Inflamm Res. 2021 Dec 8;14:6669-6670. doi: 10.2147/JIR.S352173. eCollection 2021. J Inflamm Res. 2021. PMID: 34916818 Free PMC article.
Abstract
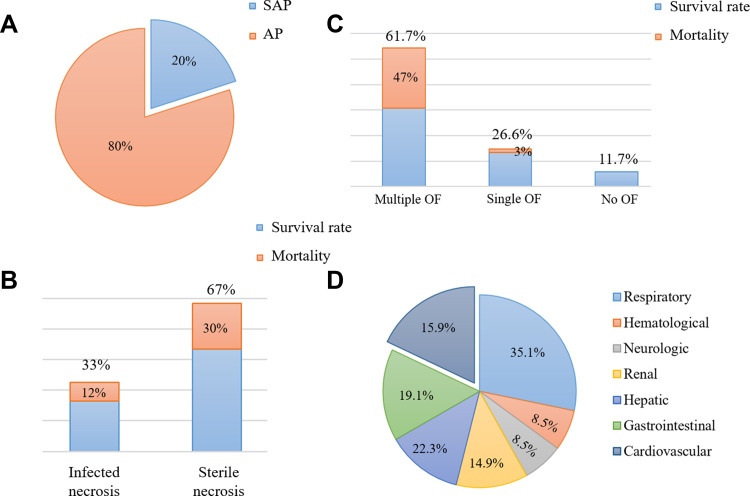
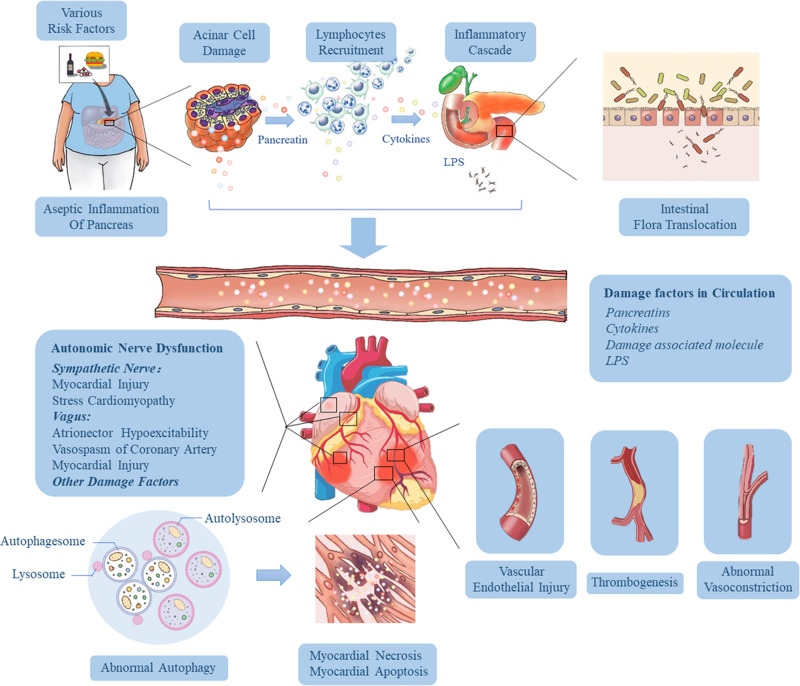
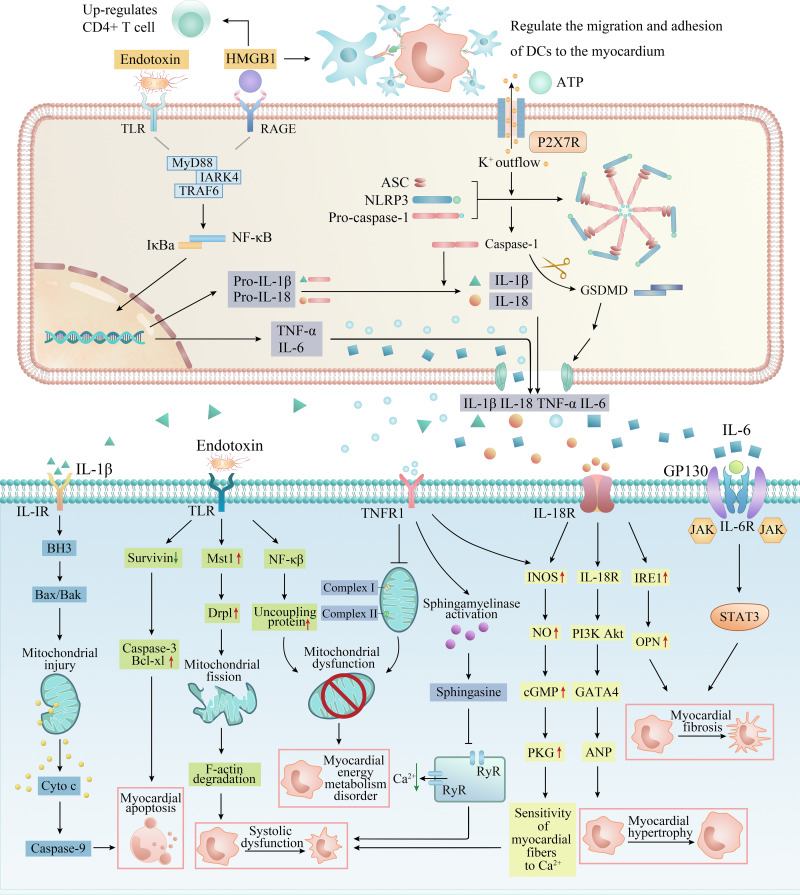
Acute pancreatitis (AP) is one of the common acute abdominal inflammatory diseases in clinic with acute onset and rapid progress. About 20% of the patients will eventually develop into severe acute pancreatitis (SAP) characterized by a large number of inflammatory cells infiltration, gland flocculus flaky necrosis and hemorrhage, finally inducing systemic inflammatory response syndrome (SIRS) and multiple organ dysfunction syndrome (MODS). Pancreatic enzyme activation, intestinal endotoxemia (IETM), cytokine activation, microcirculation disturbance, autonomic nerve dysfunction and autophagy dysregulation all play an essential role in the occurrence and progression of SAP. Organ dysfunction is the main cause of early death in SAP. Acute kidney injury (AKI) and acute lung injury (ALI) are common, while cardiac injury (CI) is not, but the case fatality risk is high. Many basic studies have observed obvious ultrastructure change of heart in SAP, including myocardial edema, cardiac hypertrophy, myocardial interstitial collagen deposition. Moreover, in clinical practice, patients with SAP often presented various abnormal electrocardiogram (ECG) and cardiac function. Cases complicated with acute myocardial infarction and pericardial tamponade have also been reported and even result in stress cardiomyopathy. Due to the molecular mechanisms underlying SAP-associated cardiac injury (SACI) remain poorly understood, and there is no complete, unified treatment and sovereign remedy at present, this article reviews reports referring to the pathogenesis, potential markers and treatment methods of SACI in recent years, in order to improve the understanding of cardiac injury in severe pancreatitis.
Keywords: biomarkers; cardiac dysfunction; cardiac injury; inflammatory mediators; severe acute pancreatitis; treatment.
© 2021 Luo et al.
Conflict of interest statement
Yalan Luo, Zhaoxia Li and Peng Ge are co-first authors. The authors declare that there are no conflicts of interest.
Figures
Similar articles
-
Intestinal barrier damage, systemic inflammatory response syndrome, and acute lung injury: A troublesome trio for acute pancreatitis.Biomed Pharmacother. 2020 Dec;132:110770. doi: 10.1016/j.biopha.2020.110770. Epub 2020 Oct 2. Biomed Pharmacother. 2020. PMID: 33011613 Review.
-
Intestinal bacterial overgrowth in the early stage of severe acute pancreatitis is associated with acute respiratory distress syndrome.World J Gastroenterol. 2021 Apr 21;27(15):1643-1654. doi: 10.3748/wjg.v27.i15.1643. World J Gastroenterol. 2021. PMID: 33958849 Free PMC article.
-
Abdominal paracentesis drainage ameliorates myocardial injury in severe experimental pancreatitis rats through suppressing oxidative stress.World J Gastroenterol. 2020 Jan 7;26(1):35-54. doi: 10.3748/wjg.v26.i1.35. World J Gastroenterol. 2020. PMID: 31933513 Free PMC article.
-
Protective effect of transplanted bone marrow-derived mesenchymal stem cells on pancreatitis-associated lung injury in rats.Mol Med Rep. 2012 Aug;6(2):287-92. doi: 10.3892/mmr.2012.922. Epub 2012 May 21. Mol Med Rep. 2012. PMID: 22613963
-
Signal Pathways and Markers Involved in Acute Lung Injury Induced by Acute Pancreatitis.Dis Markers. 2021 Aug 28;2021:9947047. doi: 10.1155/2021/9947047. eCollection 2021. Dis Markers. 2021. PMID: 34497676 Free PMC article. Review.
Cited by
-
Interpretable prediction of 30-day mortality in patients with acute pancreatitis based on machine learning and SHAP.BMC Med Inform Decis Mak. 2024 Nov 5;24(1):328. doi: 10.1186/s12911-024-02741-7. BMC Med Inform Decis Mak. 2024. PMID: 39501235 Free PMC article.
-
Pancreatitis-associated Myocarditis: Systematic Review and Meta-analysis of a Deadly Duo.J Cardiovasc Echogr. 2024 Oct-Dec;34(4):160-169. doi: 10.4103/jcecho.jcecho_59_24. Epub 2024 Dec 19. J Cardiovasc Echogr. 2024. PMID: 39895893 Free PMC article. Review.
-
Urolithin A protects severe acute pancreatitis-associated acute cardiac injury by regulating mitochondrial fatty acid oxidative metabolism in cardiomyocytes.MedComm (2020). 2023 Dec 19;4(6):e459. doi: 10.1002/mco2.459. eCollection 2023 Dec. MedComm (2020). 2023. PMID: 38116065 Free PMC article.
-
The Impact of Type 2 Myocardial Infarction in Acute Pancreatitis: Analysis of 1.1 Million Hospitalizations and Review of the Literature.Cureus. 2023 Aug 25;15(8):e44113. doi: 10.7759/cureus.44113. eCollection 2023 Aug. Cureus. 2023. PMID: 37750110 Free PMC article.
-
Assessment of frontal QRS-T angle in distinguishing mild and severe acute pancreatitis in emergency department: A retrospective study.Medicine (Baltimore). 2024 Nov 29;103(48):e40743. doi: 10.1097/MD.0000000000040743. Medicine (Baltimore). 2024. PMID: 39612376 Free PMC article.
References
-
- Lovett WL, Wangensteen SL, Glenn TM, Lefer AM. Presence of a myocardial depressant factor in patients in circulatory shock. Surgery. 1971;70:223–231. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
