

Juvenile granulosa cell tumor diagnosed in 6-month-old infant with precocious puberty
- PMID: 34285730
- PMCID: PMC8278142
- DOI: 10.1016/j.radcr.2021.06.006
Juvenile granulosa cell tumor diagnosed in 6-month-old infant with precocious puberty
Erratum in
-
Erratum to "Juvenile granulosa cell tumor diagnosed in 6-month-old infant with precocious puberty" [Radiology Case Reports 16 (2021) 2609-2613].Radiol Case Rep. 2024 May 21;19(8):3596. doi: 10.1016/j.radcr.2023.06.050. eCollection 2024 Aug. Radiol Case Rep. 2024. PMID: 39022116 Free PMC article.
Abstract
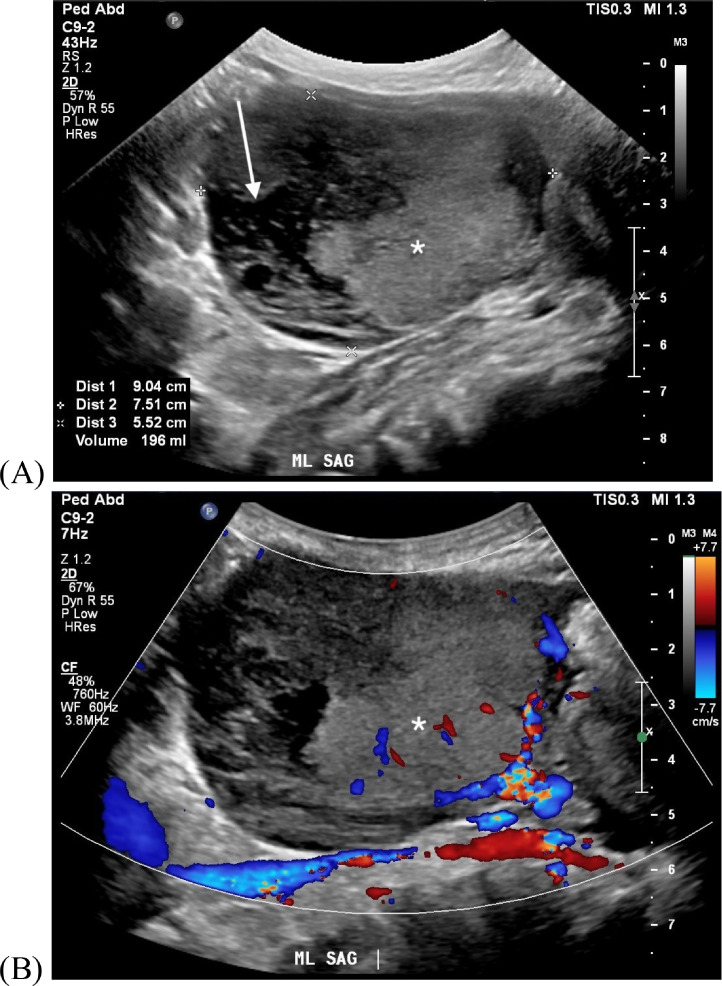
Juvenile granulosa cell tumor is a rare tumor diagnosed in children, which can present with precocious puberty. We have reported a case of a 6-month-old female patient who presented with precocious puberty. Abdominopelvic imaging revealed a large mixed cystic and solid mass, with internal solid enhancement, and restricted diffusion. At surgery, mass was confirmed to arise from the left ovary, and histopathology confirmed juvenile granulosa cell tumor. We provide a literature review of juvenile granulosa cell tumor and discuss imaging characteristics of this diagnosis.
Keywords: Juvenile granulosa cell tumor; Ovarian tumor; Precocious puberty.
© 2021 Published by Elsevier Inc. on behalf of University of Washington.
Figures



Similar articles
-
Unusual radiologic imaging in juvenile granulosa cell tumor with precocious puberty: A unilocular cyst.Radiol Case Rep. 2024 Jul 25;19(10):4283-4288. doi: 10.1016/j.radcr.2024.06.072. eCollection 2024 Oct. Radiol Case Rep. 2024. PMID: 39161564 Free PMC article.
-
Transformation of Peripheral Sexual Precocity to Central Sexual Precocity Following Treatment of Granulosa Cell Tumor of the Ovary.Cureus. 2022 Feb 28;14(2):e22676. doi: 10.7759/cureus.22676. eCollection 2022 Feb. Cureus. 2022. PMID: 35371651 Free PMC article.
-
Juvenile granulosa and theca cell tumor of the ovary as a rare cause of precocious puberty: case report and review of literature.J Pediatr Adolesc Gynecol. 2010 Aug;23(4):e127-31. doi: 10.1016/j.jpag.2010.01.003. Epub 2010 Apr 3. J Pediatr Adolesc Gynecol. 2010. PMID: 20371195 Review.
-
Juvenile granulosa cell tumor presenting as isosexual precocious puberty: A case report and review of literature.Indian J Endocrinol Metab. 2013 Jan;17(1):157-9. doi: 10.4103/2230-8210.107870. Indian J Endocrinol Metab. 2013. PMID: 23776871 Free PMC article.
-
Juvenile granulosa cell ovarian tumor: a case report and review of literature.J Pediatr Adolesc Gynecol. 2009 Oct;22(5):e114-7. doi: 10.1016/j.jpag.2008.08.001. Epub 2009 Jul 3. J Pediatr Adolesc Gynecol. 2009. PMID: 19576820 Review.
Cited by
-
Unusual radiologic imaging in juvenile granulosa cell tumor with precocious puberty: A unilocular cyst.Radiol Case Rep. 2024 Jul 25;19(10):4283-4288. doi: 10.1016/j.radcr.2024.06.072. eCollection 2024 Oct. Radiol Case Rep. 2024. PMID: 39161564 Free PMC article.
-
A Rare Case of Juvenile Granulosa Cell Tumor in a Premenarchal Female: Clinical Presentation, Diagnosis, and Management.Cureus. 2024 Dec 28;16(12):e76546. doi: 10.7759/cureus.76546. eCollection 2024 Dec. Cureus. 2024. PMID: 39877787 Free PMC article.
References
-
- Outwater W. Sex cord-stromal and steroid cell tumors of the ovary. Radiographics. 1998;18(6):1523–1546. - PubMed
-
- Zhang J. Ovarian masses in children and adolescents - an analysis of 521 clinical cases. J Pediatr Adolesc Gynecol. 2014;27(3):e73–e77. - PubMed
-
- Young D. Juvenile granulosa cell tumor of the ovary. Am J Surg Pathol. 1984;8(8):575–596. - PubMed
-
- Wu P. Juvenile granulosa cell tumor of the ovary: a clinicopathologic study. J Pediatr Adolesc Gynecol. 2016;30(1):138–143. - PubMed
-
- Merras-Salmio V. Ovarian granulosa cell tumors in childhood. Pediatr Hematol Oncol. 2002;19(3):145–156. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
