

Abdominal Pain Caused by Occlusion of the Celiac Trunk and Superior Mesenteric Artery in Addition to Irritable Bowel Syndrome: Case Series and Literature Review
- PMID: 34285841
- PMCID: PMC8286357
- DOI: 10.7759/cureus.15729
Abdominal Pain Caused by Occlusion of the Celiac Trunk and Superior Mesenteric Artery in Addition to Irritable Bowel Syndrome: Case Series and Literature Review
Abstract
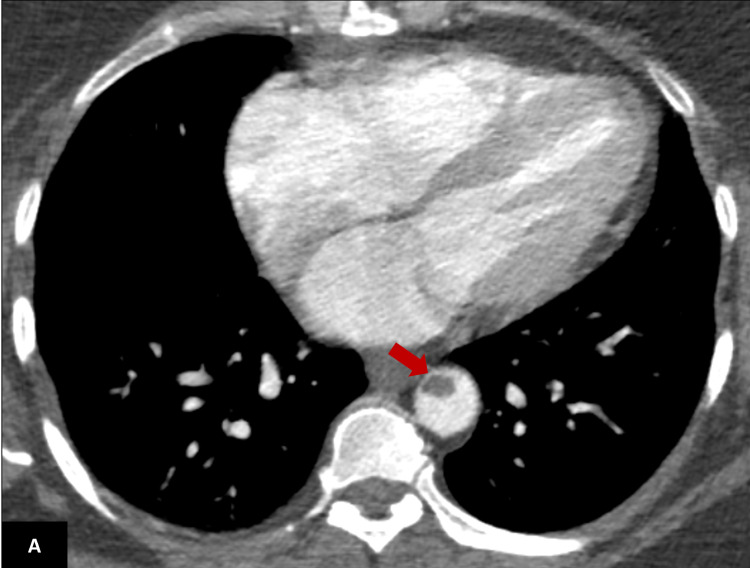
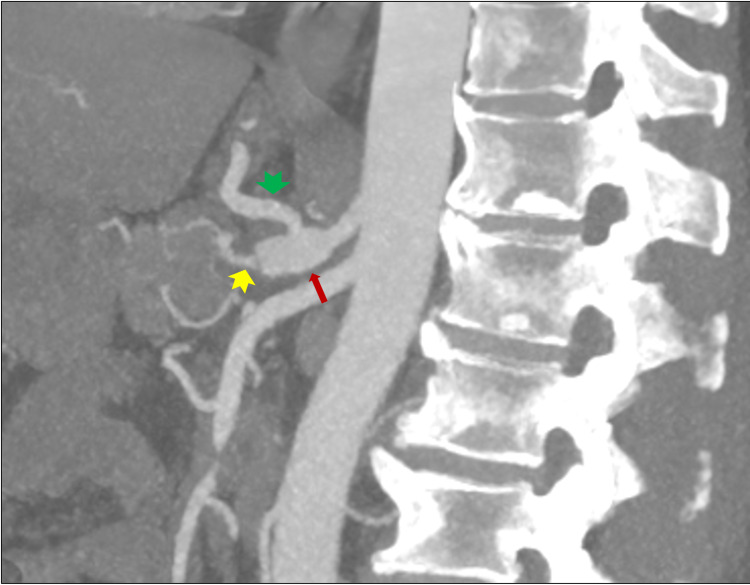
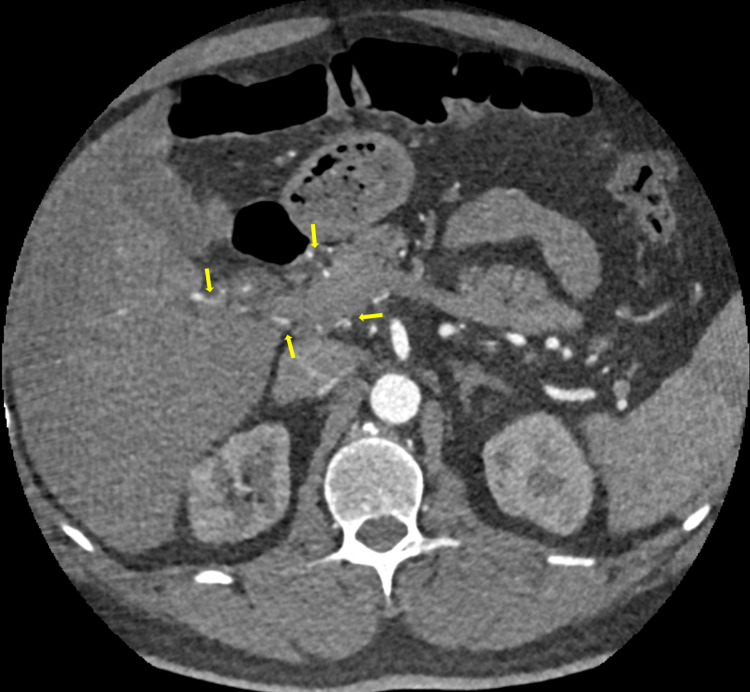
Irritable bowel syndrome (IBS) is a benign condition of the gastrointestinal tract causing abdominal pain, bloating, diarrhea, and/or constipation. Symptoms of IBS usually improve on passing flatus and defecation. There is no known identifiable underlying pathology; however, several risk factors are known to contribute to the development of IBS, which include a stressful lifestyle and certain foods such as bread, coffee, alcohol, pasta, and chocolates. Intestinal bacteria may also contribute to symptoms of IBS. IBS is diagnosed clinically and treated with various medications to control the symptoms. On the other hand, celiac and mesenteric artery thrombosis (CAMAT) is a condition that may cause significantly higher mortality and morbidity if not recognized early. CAMAT leads to the blockage of major blood vessels to the intestine and several abdominal viscera leading to abdominal pain, nausea, sweating, and, in some cases, symptoms of shock. CAMAT is most likely caused by thrombosis; however, occasionally, embolisms from distant sources in patients with atrial fibrillation can also contribute to the development of CAMAT. CAMAT is usually diagnosed with a computed tomography angiogram (CTA) and treated either surgically or medically with anticoagulants. Vascular thrombus in the thoracic and abdominal region causing ischemia of the stomach and abdominal pain in patients with a history of IBS can easily be missed and cause grave complications with high morbidity and mortality. We present two cases who were initially diagnosed and treated for IBS and later diagnosed with serious intra-abdominal pathology of CAMAT thrombosis. The first case is of a 55-year-old female who was previously diagnosed with IBS and was treated with mebeverine 200mg twice daily and esomeprazole 20mg once daily for 10 weeks. Her pain continued to get worse and she presented to the emergency department by ambulance. She underwent CTA, which showed occlusion of the celiac trunk and superior mesenteric artery causing liver and splenic infarcts. The patient received heparin and underwent a thrombectomy and embolectomy of the superior mesenteric and celiac arteries. No significant abnormality was found in the blood results. Thrombophilia screening was negative. The patient was discharged on warfarin. The second case is of a 53-year-old man who was also initially diagnosed with IBS and was treated with mebeverine 200mg twice daily for eight weeks before presenting to the emergency department with worsening abdominal pain. He underwent a CTA with contrast, which showed occlusion of the common hepatic artery and stenosis of the splenic artery leading to multiple splenic infarcts. No significant abnormality was found in blood test. Thrombophilia screening was negative. He was treated with new anticoagulant medication, dabigatran 150 mg orally twice daily. Both patients were managed with successful outcomes and were discharged home on anticoagulants. There was no recurrence of symptoms at three-month follow-up. These cases highlight that a secondary cause of symptoms such as vascular thrombosis must be sought for patients who fail to improve with conservative management of IBS.
Keywords: abdominal pain; irritable bowel syndrome; mesenteric ischemia; sma occlusion; splenic infarcts; vascular thrombosis.
Copyright © 2021, Khuda Bakhsh et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Irritable bowel syndrome: epidemiology, pathophysiology, Diagnosis, And Treatment. Defrees DN, Bailey J. Prim Care. 2017;44:655–671. - PubMed
-
- New insights into the pathogenesis and treatment of irritable bowel syndrome. Oświęcimska J, Szymlak A, Roczniak W, Girczys-Połedniok K, Kwiecień J. Adv Med Sci. 2017;62:17–30. - PubMed
Publication types
LinkOut - more resources
Full Text Sources