

Propensity Score Matching Analysis of the Effect of Payer Status on the Survival of Colon Cancer Patients
- PMID: 34285854
- PMCID: PMC8286796
- DOI: 10.7759/cureus.15748
Propensity Score Matching Analysis of the Effect of Payer Status on the Survival of Colon Cancer Patients
Abstract
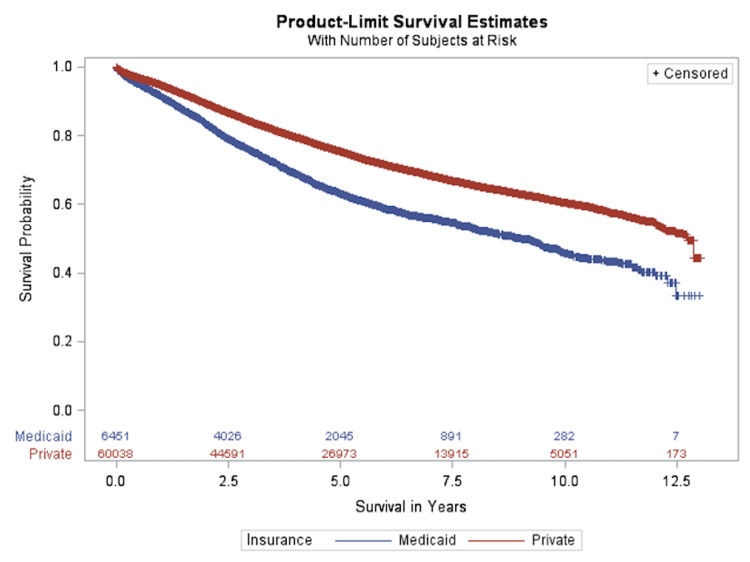
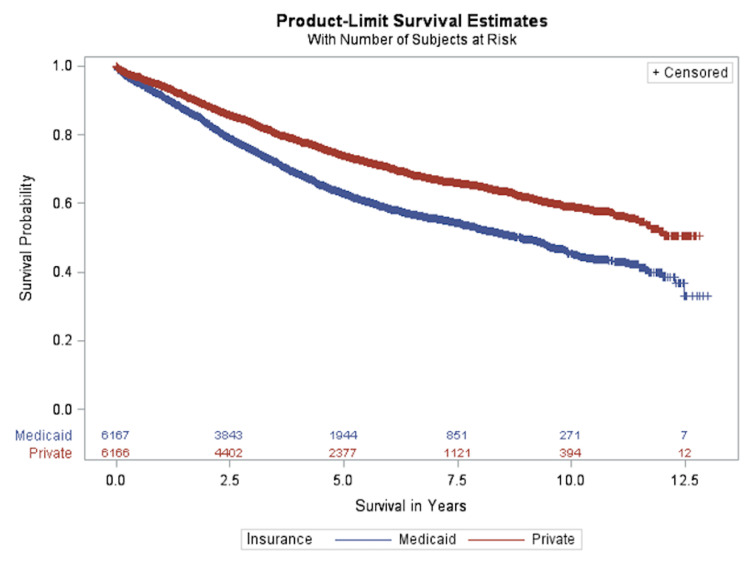
Background and objective Colon cancer is one of the most common types of cancer globally. The factors that could affect colon cancer survival include age, stage, treatment, and other socioeconomic aspects. Payer status has been shown to be a significant predictor of cancer patient survival in retrospective studies. However, due to the limitations of retrospective studies, patient baseline characteristics between payer statuses are not comparable. Few studies have addressed the effect of payer status on the overall survival (OS) of patients using propensity score matching (PSM). In light of this, we conducted a study to examine the effect of payer status on the survival of colon cancer patients based on PSM. Materials and methods About 66,493 stage II/III colon cancer patients aged 40-90 years and diagnosed between 2004 and 2015 were analyzed from a de-identified National Cancer Database (NCDB) file. All patients had undergone surgery, and patients who had received radiation therapy, hormone therapy, immunotherapy, palliative care, or therapies other than chemotherapy were excluded. Only private or Medicaid payer status was included. The propensity score was calculated by computing the probability of patients being in the Medicaid group using logistic regression. The PSMATCH procedure in the SAS software (SAS Inc., Gary, NC) was used to perform PSM on patients with Medicaid and private insurance. The greedy nearest neighbor matching method was used to match one Medicaid to one privately insured patient with a caliper of 0.2. At the same time, an exact match was done for gender, age group, race, and stage at diagnosis. Multivariate Cox regression was then used to estimate the effect of payer status on survival before and after PSM. Results Among the 66,493 patients, 90.3% were privately insured and 9.7% had Medicaid. In univariate analysis, payer status was found to be a significant predictor of OS. Prior to PSM, the median overall survival (MOS) for patients with private insurance was 12.75 years, while those with Medicaid had a MOS of 9.02 years. After PSM, 6,167 paired patients were matched, and patients with private insurance had a MOS of >12.82 years and Medicaid patients had a MOS of 8.88 years. After PSM, patients with Medicaid had a 50% increased risk of death, and payer status proved to be a statistically significant predictor of OS of colon cancer. Conclusion Based on our findings, as per the PSM method, payer status can be a significant predictor of survival among colon cancer patients. Also, chemotherapy, race, age, and other socioeconomic factors were also found to be significant predictors of OS. Further research should be conducted to investigate other covariates not studied here and the mediation effect of payer on the survival of cancer patients.
Keywords: colon cancer; healthcare insurance; payer status; propensity score matching (psm); retrospective study.
Copyright © 2021, Shi et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Effect of Chemotherapy Treatment on Overall Survival of Colon Cancer Patients Using Propensity Score Matching.Cureus. 2025 May 11;17(5):e83892. doi: 10.7759/cureus.83892. eCollection 2025 May. Cureus. 2025. PMID: 40497185 Free PMC article.
-
The Effect of Payer Status on Survival of Patients with Stage I/II Non-small Cell Lung Cancer: NCDB 1998-2011.Anticancer Res. 2016 Jan;36(1):319-26. Anticancer Res. 2016. PMID: 26722060
-
The Effect of Payer Status on Survival of Patients With Prostate Cancer.Cureus. 2021 Feb 13;13(2):e13329. doi: 10.7759/cureus.13329. Cureus. 2021. PMID: 33738172 Free PMC article.
-
Characteristics of Hospital Stays for Super-Utilizers by Payer, 2012.2015 May. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006 Feb–. Statistical Brief #190. 2015 May. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006 Feb–. Statistical Brief #190. PMID: 26247093 Free Books & Documents. Review.
-
Propensity score matching with R: conventional methods and new features.Ann Transl Med. 2021 May;9(9):812. doi: 10.21037/atm-20-3998. Ann Transl Med. 2021. PMID: 34268425 Free PMC article. Review.
Cited by
-
Closing the Gap: Approaches to Improving Colorectal Surgery Care for the Uninsured and Underinsured.Clin Colon Rectal Surg. 2024 May 15;38(1):49-57. doi: 10.1055/s-0044-1786398. eCollection 2025 Jan. Clin Colon Rectal Surg. 2024. PMID: 39734719 Free PMC article. Review.
-
Effect of Chemotherapy Treatment on Overall Survival of Colon Cancer Patients Using Propensity Score Matching.Cureus. 2025 May 11;17(5):e83892. doi: 10.7759/cureus.83892. eCollection 2025 May. Cureus. 2025. PMID: 40497185 Free PMC article.
References
-
- Association of insurance with cancer care utilization and outcomes. Ward E, Halpern M, Schrag N, et al. CA Cancer J Clin. 2008;58:9–31. - PubMed
-
- Contribution of income-related inequality and healthcare utilisation to survival in cancers of the lung, liver, stomach and colon. Yim J, Hwang SS, Yoo KY, Kim CY. J Epidemiol Community Health. 2012;66:37–40. - PubMed
-
- The effect of health insurance status on the treatment and outcomes of patients with colorectal cancer. Parikh AA, Robinson J, Zaydfudim VM, Penson D, Whiteside MA. J Surg Oncol. 2014;110:227–232. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous