

Contribution of hypercapnia to cognitive impairment in severe sleep-disordered breathing
- PMID: 34286691
- PMCID: PMC8807902
- DOI: 10.5664/jcsm.9558
Contribution of hypercapnia to cognitive impairment in severe sleep-disordered breathing
Abstract
Study objectives: Although cognitive impairment in obstructive sleep apnea (OSA) is primarily attributed to intermittent hypoxemia and sleep fragmentation, hypercapnia may also play a role in patients whose OSA is complicated by hypoventilation. This study investigated the impact of hypercapnia on cognitive function in severe sleep-disordered breathing (OSA accompanied by hypoventilation).
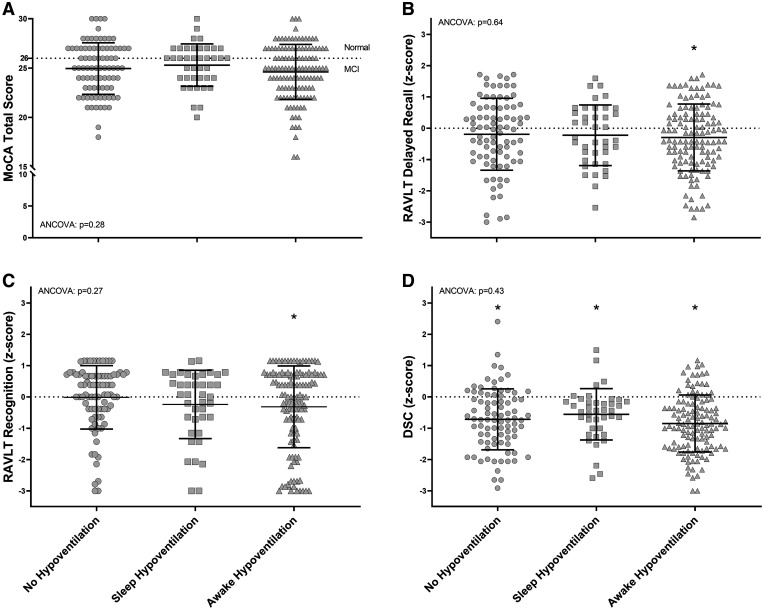
Methods: Patients with severe OSA (apnea-hypopnea index >30 events/h; n = 246) underwent evaluation for accompanying hypoventilation with polysomnography that included continuous transcutaneous carbon dioxide (TcCO2) monitoring and awake arterial blood gas analysis. Patients were categorized as having no hypoventilation (n = 84), isolated sleep hypoventilation (n = 40), or awake hypoventilation (n = 122). Global cognitive function was evaluated using the Montreal Cognitive Assessment (MoCA), memory with the Rey Auditory Verbal Learning Test (RAVLT), and processing speed with the Wechsler Adult Intelligence Scale, Fourth Edition (WAIS-IV), Digit Symbol Coding subtest (DSC).
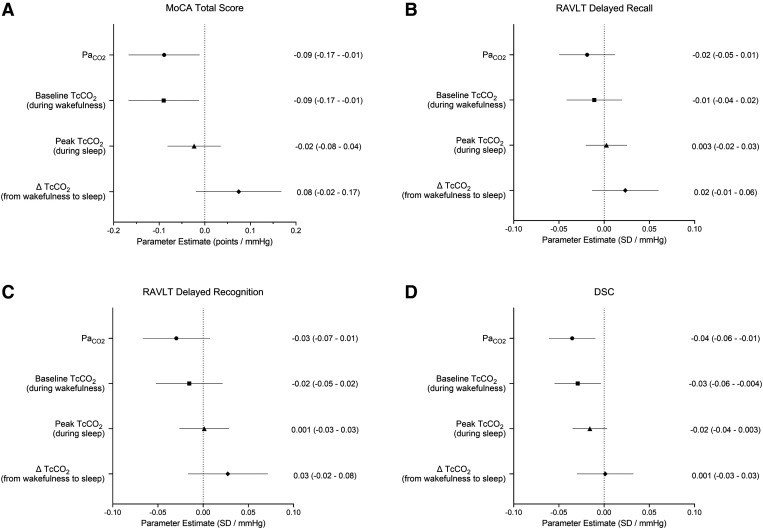
Results: Apnea-hypopnea index was similar across groups (P = .15), but the sleep and awake hypoventilation groups had greater nocturnal hypoxemia compared with the no-hypoventilation group (P < .01). Within all groups, mean MoCA scores were < 26, which is the validated threshold to indicate mild cognitive impairment; RAVLT scores were lower than age-matched norms only in the awake-hypoventilation group (P ≤ .01); and DSC scores were lower than age-matched norms within all groups (P < .01). In multivariable regression analyses, higher arterial partial pressure of carbon dioxide (PaCO2) and TcCO2 during wakefulness were associated with lower MoCA and DSC scores (P ≤ .03), independent of confounders including overlap syndrome (OSA + chronic obstructive pulmonary disease).
Conclusions: Awake hypoventilation is associated with greater deficits in cognitive function in patients with severe sleep-disordered breathing.
Citation: Beaudin AE, Raneri JK, Ayas NT, Skomro RP, Smith EE, Hanly PJ; on behalf of Canadian Sleep and Circadian Network. Contribution of hypercapnia to cognitive impairment in severe sleep-disordered breathing. J Clin Sleep Med. 2022;18(1):245-254.
Keywords: cognitive function; hypercapnia; hypoventilation syndrome; sleep-disordered breathing.
© 2022 American Academy of Sleep Medicine.
Conflict of interest statement
All authors have seen and approved the manuscript. A.E.B was supported by postdoctoral fellowships from the Canadian Alzheimer Association & Canadian Consortium on Neurodegeneration in Aging (CCNA), Campus Alberta Neuroscience, and the Canadian Institutes of Health Research (CIHR); and funds from a Brain Canada operating grant. J.K.R. was supported by funds from the Cumming School of Medicine, Sleep Research Program (University of Calgary), and the Canadian Sleep and Circadian Network (CSCN). E.E.S. holds the Katthy Taylor Chair in Vascular Dementia from the University of Calgary. This study was funded by the CSCN, which is funded through a CIHR Community Development Program grant. R.P.S. reports that they have provided consulting work to ResMed, GSK, and AstraZeneca outside the submitted work. The other authors report no conflicts of interest.
Figures
References
-
- Bucks RS, Olaithe M, Eastwood P. Neurocognitive function in obstructive sleep apnoea: a meta-review. Respirology. 2013; 18( 1): 61– 70. - PubMed
-
- Gagnon K, Baril AA, Gagnon JF, et al. . Cognitive impairment in obstructive sleep apnea. Pathol Biol (Paris). 2014; 62( 5): 233– 240. - PubMed
-
- Champod AS, Eskes GA, Foster GE, et al. . Effects of acute intermittent hypoxia on working memory in young healthy adults. Am J Respir Crit Care Med. 2013; 187 ( 10): 1148– 1150. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
