

Durable Antibody Responses in Staff at Two Long-Term Care Facilities, during and Post SARS-CoV-2 Outbreaks
- PMID: 34287058
- PMCID: PMC8552744
- DOI: 10.1128/Spectrum.00224-21
Durable Antibody Responses in Staff at Two Long-Term Care Facilities, during and Post SARS-CoV-2 Outbreaks
Abstract
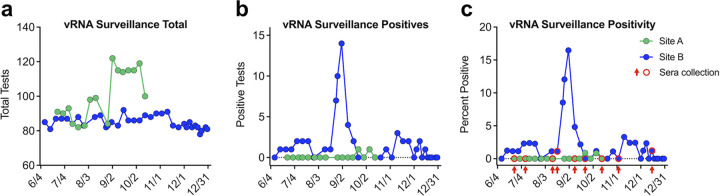
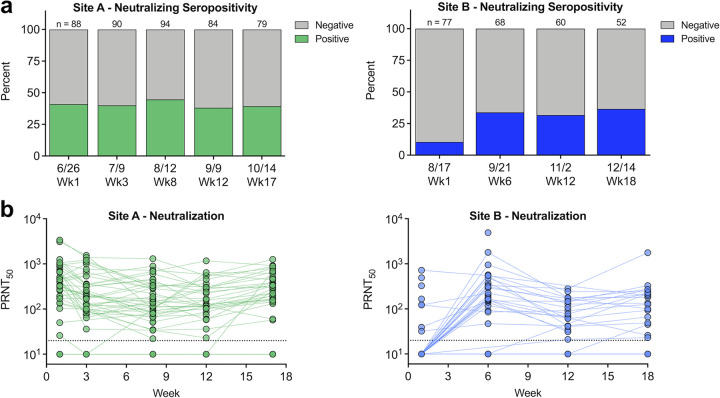
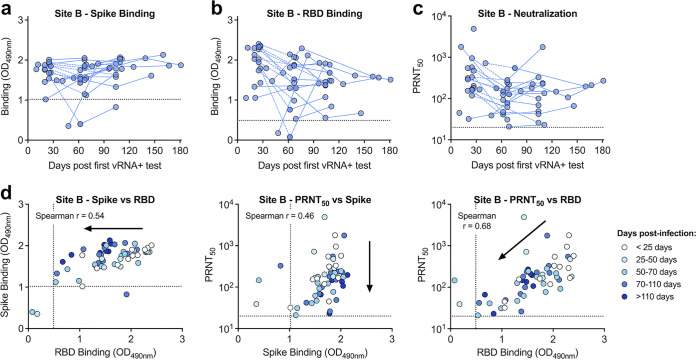
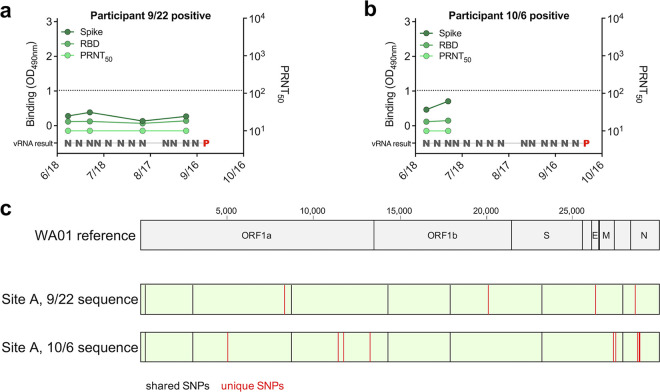
SARS-CoV-2 has had a disproportionate impact on nonhospital health care settings, such as long-term-care facilities (LTCFs). The communal nature of these facilities, paired with the high-risk profile of residents, has resulted in thousands of infections and deaths and a high case fatality rate. To detect presymptomatic infections and identify infected workers, we performed weekly surveillance testing of staff at two LTCFs, which revealed a large outbreak at one of the sites. We collected serum from staff members throughout the study and evaluated it for binding and neutralization to measure seroprevalence, seroconversion, and type and functionality of antibodies. At the site with very few incident infections, we detected that over 40% of the staff had preexisting SARS-CoV-2 neutralizing antibodies, suggesting prior exposure. At the outbreak site, we saw rapid seroconversion following infection. Neutralizing antibody levels were stable for many weeks following infection, suggesting a durable, long-lived response. Receptor-binding domain antibodies and neutralizing antibodies were strongly correlated. The site with high seroprevalence among staff had two unique introductions of SARS-CoV-2 into the facility through seronegative infected staff during the period of study, but these did not result in workplace spread or outbreaks. Together, our results suggest that a high seroprevalence rate among staff can contribute to immunity within a workplace and protect against subsequent infection and spread within a facility. IMPORTANCE Long-term care facilities (LTCFs) have been disproportionately impacted by COVID-19 due to their communal nature and high-risk profile of residents. LTCF staff have the ability to introduce SARS-CoV-2 into the facility, where it can spread, causing outbreaks. We tested staff weekly at two LTCFs and collected blood throughout the study to measure SARS-CoV-2 antibodies. One site had a large outbreak and infected individuals rapidly generated antibodies after infection. At the other site, almost half the staff already had antibodies, suggesting prior infection. The majority of these antibodies bind to the receptor-binding domain of the SARS-CoV-2 spike protein and are potently neutralizing and stable for many months. The non-outbreak site had two unique introductions of SARS-CoV-2 into the facility, but these did not result in workplace spread or outbreaks. Our results reveal that high seroprevalence among staff can contribute to immunity and protect against subsequent infection and spread within a facility.
Keywords: adaptive immunity; coronavirus; neutralizing antibodies; surveillance studies.
Figures


References
-
- Centers for Medicare & Medicaid Services. 2020. The nursing home COVID-19 public file. https://data.cms.gov/stories/s/COVID-19-Nursing-Home-Data/bkwz-xpvg/. - PubMed
-
- New York Times. 2020. More than 40% of U.S. coronavirus deaths are linked to nursing homes. https://www.nytimes.com/interactive/2020/us/coronavirus-nursing-homes.html.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
