

Neurological and Head/Eyes/Ears/Nose/Throat Manifestations of COVID-19: A Systematic Review and Meta-Analysis
- PMID: 34287109
- PMCID: PMC8460425
- DOI: 10.1017/cjn.2021.180
Neurological and Head/Eyes/Ears/Nose/Throat Manifestations of COVID-19: A Systematic Review and Meta-Analysis
Abstract
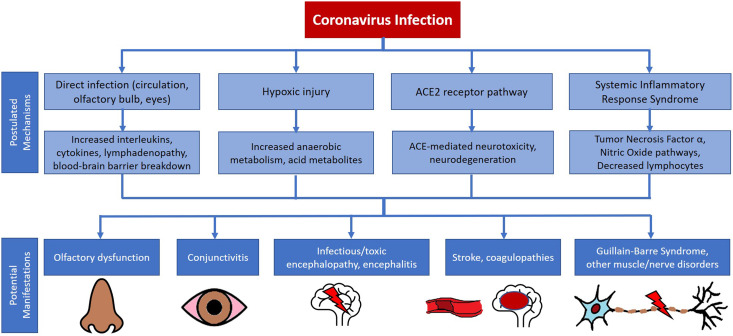
Background/objective: Coronavirus disease 2019 (COVID-19) has been associated with various neurological and atypical head/eyes/ears/nose/throat (HEENT) manifestations. We sought to review the evidence for these manifestations.
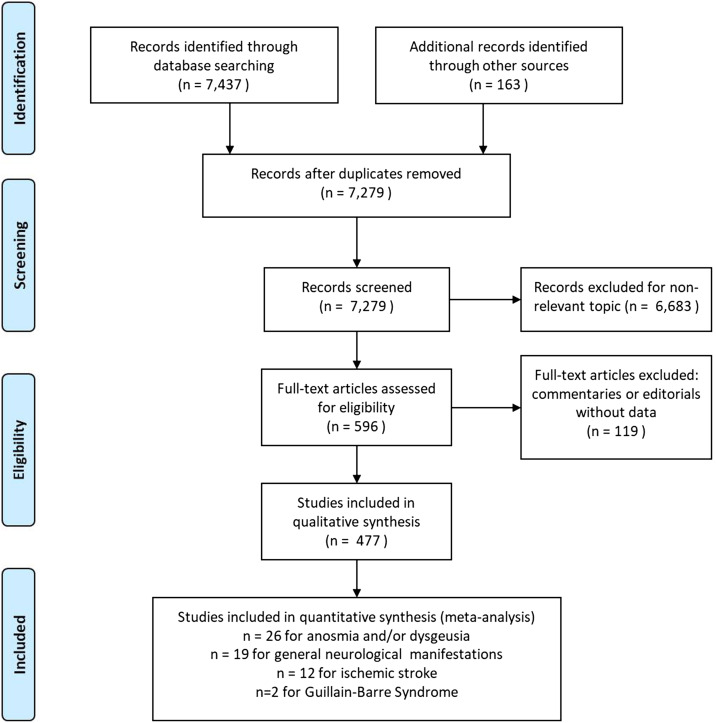
Methods: In this systematic review and meta-analysis, we compiled studies published until March 31, 2021 that examined non-respiratory HEENT, central, and peripheral nervous system presentations in COVID-19 patients. We included 477 studies for qualitative synthesis and 59 studies for meta-analyses.
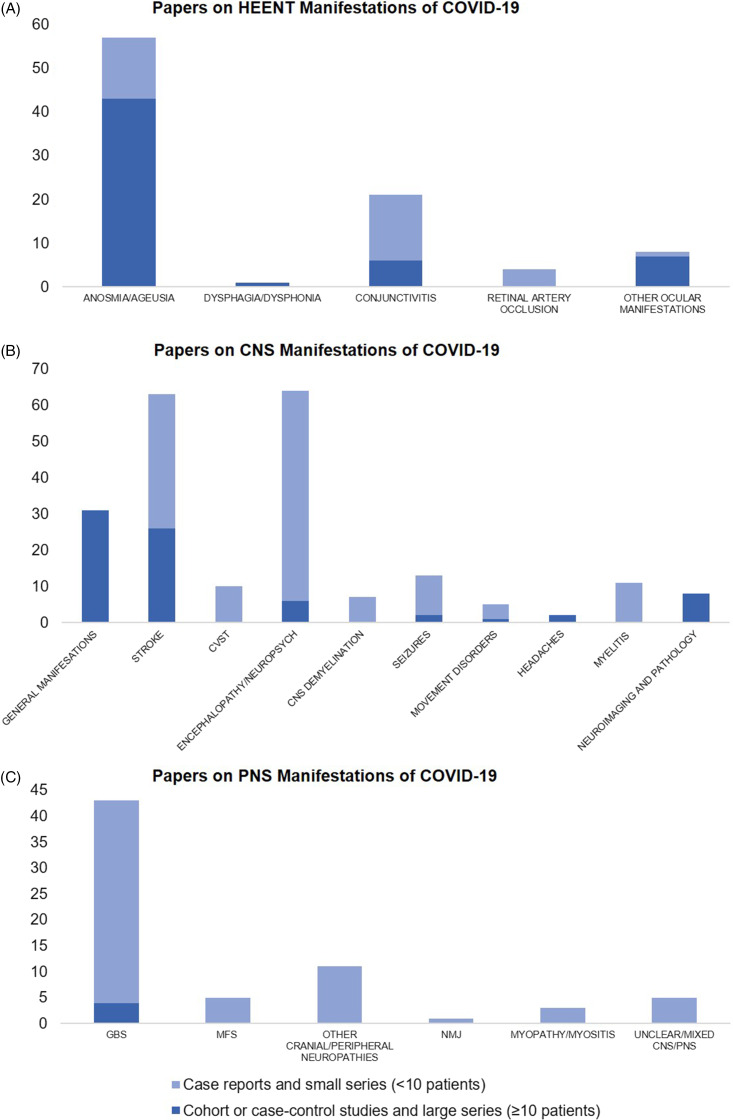
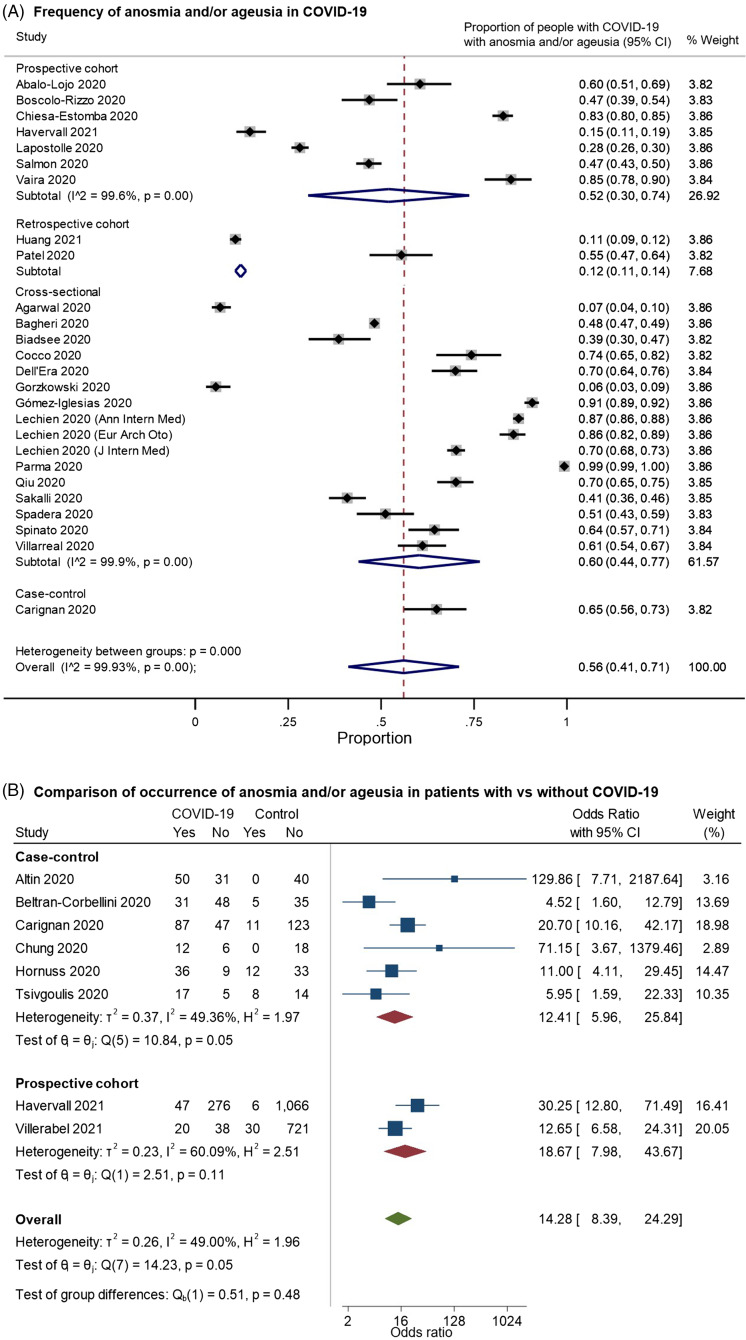
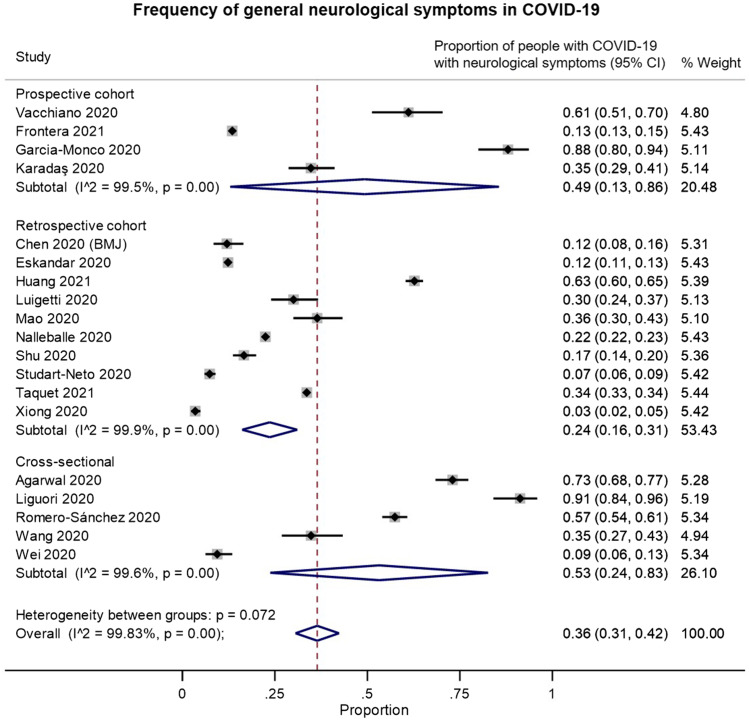
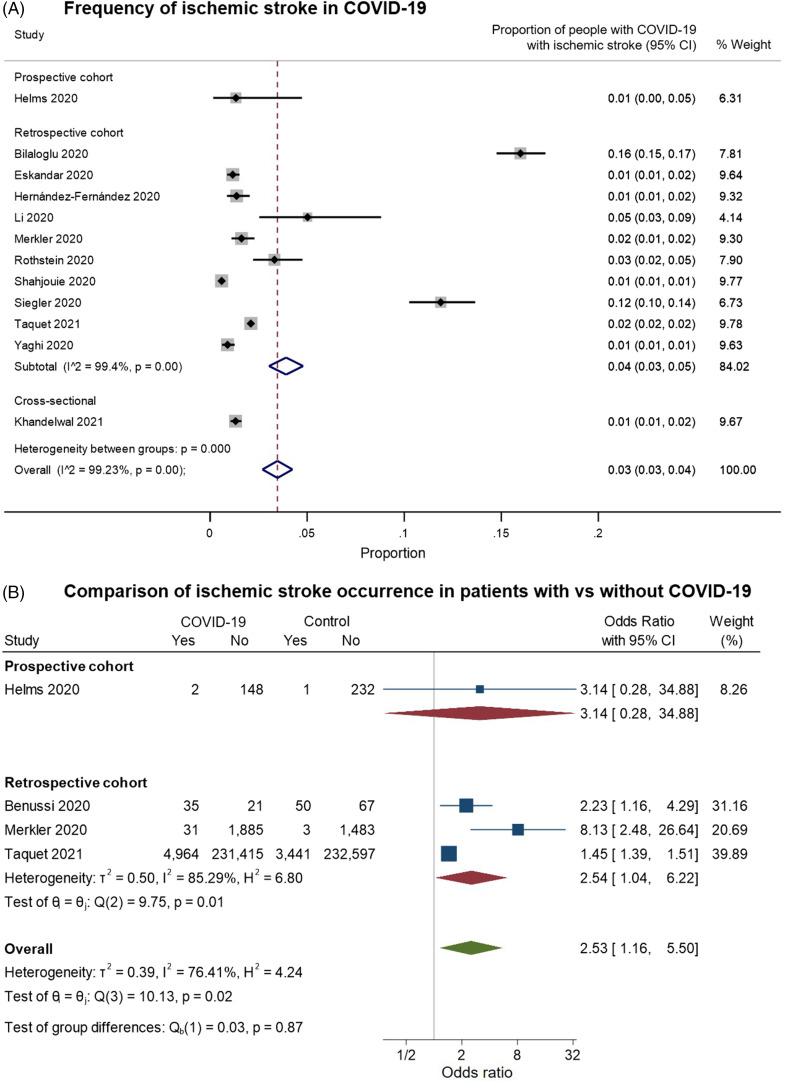
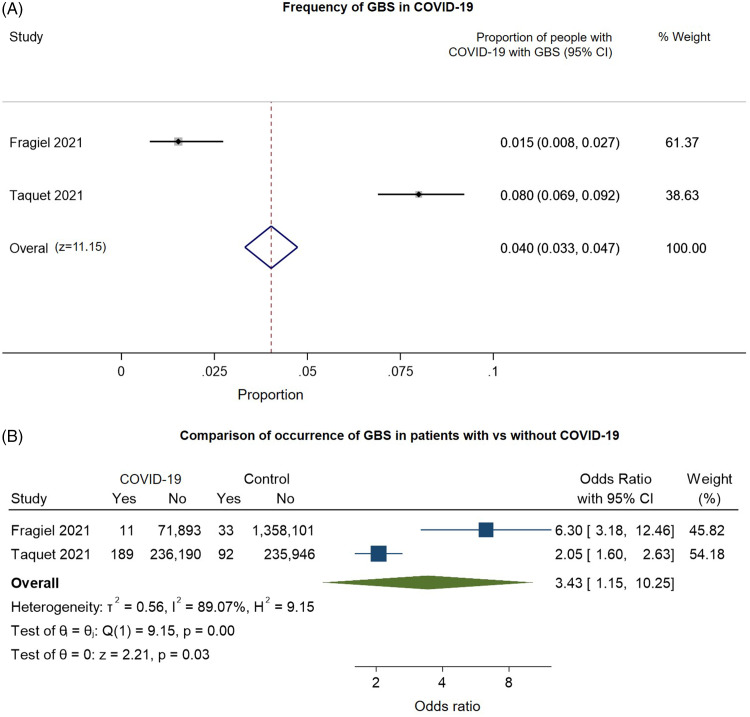
Results: Anosmia, ageusia, and conjunctivitis may precede typical upper/lower respiratory symptoms. Central nervous system (CNS) manifestations include stroke and encephalopathy, potentially with brainstem or cranial nerve involvement. MRI studies support CNS para-/postinfectious etiologies, but direct neuroinvasion seems very rare, with few cases detecting Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in the CNS. Peripheral nervous system (PNS) manifestations include muscle damage, Guillain-Barre syndrome (GBS), and its variants. There was moderate-to-high study heterogeneity and risk of bias. In random-effects meta-analyses, anosmia/ageusia was estimated to occur in 56% of COVID-19 patients (95% CI: 0.41-0.71, I2:99.9%), more commonly than in patients without COVID-19 (OR: 14.28, 95% CI: 8.39-24.29, I2: 49.0%). Neurological symptoms were estimated to occur in 36% of hospitalized patients (95% CI: 0.31-0.42, I2: 99.8%); ischemic stroke in 3% (95% CI: 0.03-0.04, I2: 99.2%), and GBS in 0.04% (0.033%-0.047%), more commonly than in patients without COVID-19 (OR[stroke]: 2.53, 95% CI: 1.16-5.50, I2: 76.4%; OR[GBS]: 3.43,1.15-10.25, I2: 89.1%).
Conclusions: Current evidence is mostly from retrospective cohorts or series, largely in hospitalized or critically ill patients, not representative of typical community-dwelling patients. There remains a paucity of systematically gathered prospective data on neurological manifestations. Nevertheless, these findings support a high index of suspicion to identify HEENT/neurological presentations in patients with known COVID-19, and to test for COVID-19 in patients with such presentations at risk of infection.
Manifestations neurologiques et atypiques dans des cas d’infection à la COVID-19 : un examen systématique et une méta-analyse.
Contexte/Objectif :: Les infections à la COVID-19 ont été associées à de multiples manifestations neurologiques mais aussi à des atteintes atypiques à la tête, aux yeux, aux oreilles, aux voies nasales et à la gorge (TYOVG). Nous avons ainsi cherché à examiner les preuves de ces manifestations et de ces atteintes.
Méthodes :: Dans le cadre de cet examen systématique et de cette méta-analyse, nous avons compilé des études parues jusqu’au 31 mars 2021. Ces études s’étaient penchées sur des atteintes non-respiratoires de type TYOVG ainsi que sur des atteintes au système nerveux central (SNC) et au système périphérique (SP) chez des patients atteints d’une infection à la COVID-19. Pour ce faire, nous avons inclus 477 études de synthèse qualitatives de même que 59 études constituant des méta-analyses.
Résultats :: Il est donc possible que des manifestations d’anosmie, d’agueusie et de conjonctivite précèdent les symptômes typiques qui affectent les voies respiratoires supérieures et inférieures. Quant aux atteintes du SNC, elles ont inclus des AVC et des cas d’encéphalopathie comportant potentiellement une atteinte du tronc cérébral ou des nerfs crâniens. Des études basées sur des examens d’IRM ont certes confirmé des étiologies para et post-infectieuses du SNC ; toutefois, une neuro-invasion directe semble être largement inusitée car seulement quelques cas de coronavirus 2 (syndrome respiratoire aigu sévère) ont été détectés dans le SNC. Des atteintes au SP ont inclus par ailleurs des dommages musculaires en plus de l’apparition du syndrome de Guillain-Barré (SGB) et de ses variantes. Soulignons aussi que l’hétérogénéité des études et le risque de biais étaient modérés à élevés. Dans des méta-analyses à effets aléatoires, il a été estimé que l’anosmie et l’agueusie survenaient chez 56 % des patients atteints d’une infection à la COVID-19 (IC 95 % : 0,41–0,71, I2 : 99,9 %), ce qui est plus fréquent que chez des patients n’en étant pas atteints (RC : 14,28 ; IC 95 % : 8,39–24,29 ; I2 : 49,0 %). On estime que des symptômes de nature neurologique sont survenus chez 36 % des patients hospitalisés (IC 95 % : 0,31–0,42 ; I2 : 99,8 %) ; des AVC ischémiques chez 3 % d’entre eux (IC 95 % : 0,03–0,04 ; I2 : 99,2 %) ; et des manifestations du SGB chez 0,04 % d’entre eux (0,033–0,047 %). Encore une fois, cela est plus fréquent que chez des patients n’étant pas atteints d’une infection à la COVID-19 (RC [AVC] : 2,53 ; IC 95 % : 1,16–5,50 et I2 : 76,4 % ; RC [SGB] : 3,43 ; IC 95 % : 1,15–10,25 et I2 : 89,1 %).
Conclusions :: Les données actuelles proviennent essentiellement de cohortes ou de séries rétrospectives, principalement des patients hospitalisés ou gravement malades. Elles ne sont donc pas représentatives de patients typiques vivant en communauté. Qui plus est, les données prospectives recueillies systématiquement au sujet des manifestations neurologiques restent rares. Néanmoins, nos constatations nous portent à rester éminemment prudents dans l’identification de manifestations neurologiques et d’atteintes de type TYOVG chez des patients dont une infection à la COVID-19 est connue et en ce qui regarde la nécessité de passer un test de dépistage.
Keywords: COVID-19; Guillain–Barre; Neurology – General; Peripheral Neuropathy; Sensory systems; Stroke.
Figures
References
-
- Fan CK, Yieh KM, Peng MY, Lin JC, Wang NC, Chang FY.Clinical and laboratory features in the early stage of severe acute respiratory syndrome. J Microbiol Immunol Infect. 2006;39:45–53. - PubMed
-
- Tsai LK, Hsieh ST, Chao CC, et al. Neuromuscular disorders in severe acute respiratory syndrome. Arch Neurol. 2004;61:1669–73. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
