

Clinical Mortality Review of COVID-19 Patients at Sukraraj Tropical and Infectious Disease Hospital, Nepal; A Retrospective Study
- PMID: 34287389
- PMCID: PMC8293465
- DOI: 10.3390/tropicalmed6030137
Clinical Mortality Review of COVID-19 Patients at Sukraraj Tropical and Infectious Disease Hospital, Nepal; A Retrospective Study
Abstract
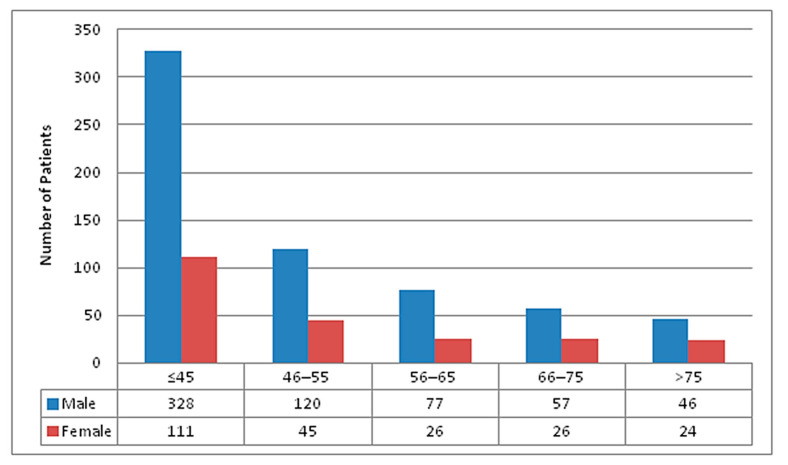
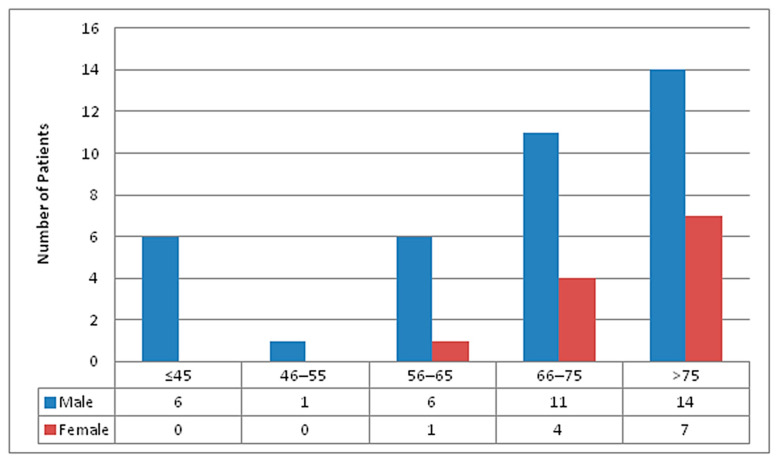
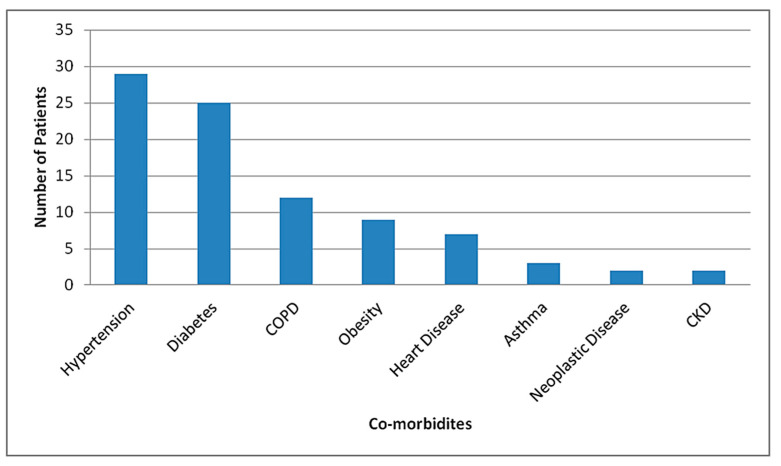
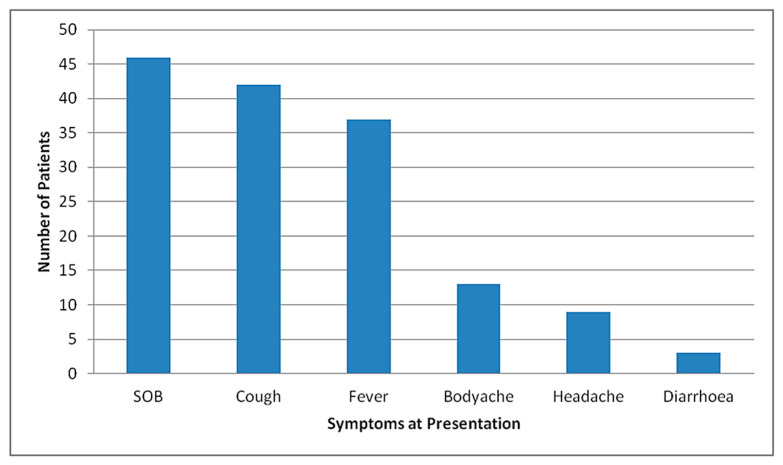
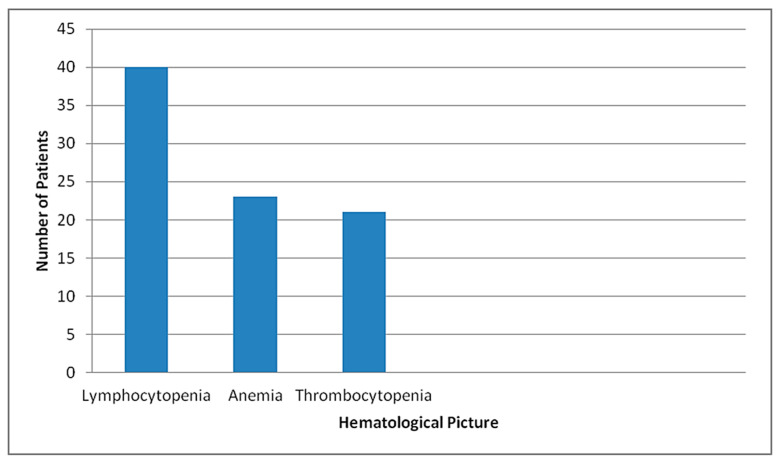
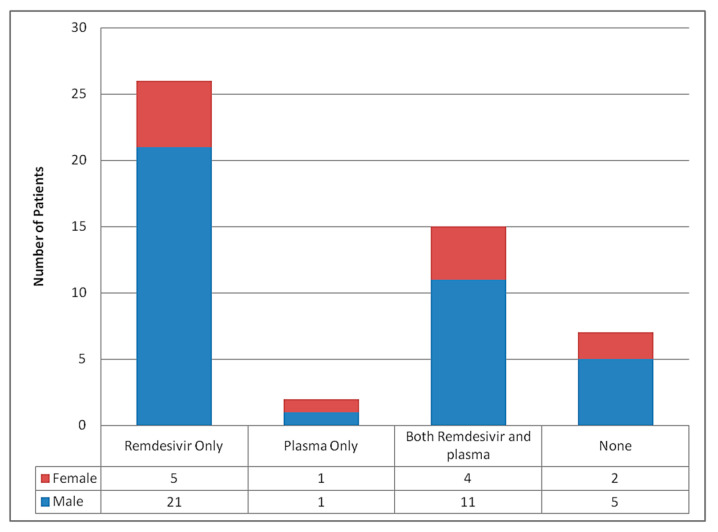
Coronavirus Disease 2019 (COVID-19) has challenged the health system worldwide, including the low and middle income countries like Nepal. In view of the rising number of infections and prediction of multiple waves of this disease, mortalities due to COVID-19 need to be critically analyzed so that every possible effort could be made to prevent COVID-19 related mortalities in future. Main aim of this research was to study about the mortalities due to COVID-19 at a tertiary level hospital, in Nepal. This was a retrospective, observational study that included all inpatients from Sukraraj Tropical and Infectious Disease Hospital, who were reverse transcriptase polymerase chain reaction positive for SARS-COV-2 and died during hospital stay from January 2020 till January 2021. Medical records of the patients were evaluated. Out of 860 total admissions in a year, there were 50 mortalities in the study center. Out of 50 mortalities, majority were males (76%) with male to female ratio of 3.17:1. Most were above 65 years of age (72%) and had two or more comorbidities (64%). The most common comorbidities among the patients who had died during hospital stay were hypertension (58%) followed by diabetes mellitus (50%) and chronic obstructive airway disease (24%). The median duration from the symptom onset to death was 18 days, ranged from the minimum of 2 days till maximum of 39 days. D-dimer was found to be >1 mg/L in 58% cases and ferritin was >500 ng/ml in 42% patients at presentation. A total of 42% patients had thrombocytopenia, 80% patients had lymphocytopenia and 60% had Neutrophil to Lymphocyte ratio >11.75 with the mean NLR of 18.38. Of total mortalities, 16% patients also showed microbiological evidence of secondary infection; Male gender, age more than 65 years, multiple comorbidities with lymphocytopenia, elevated Neutrophil lymphocyte ratio and elevated inflammatory markers were risk factors found in majority of mortalities in our study. These findings could be utilized for early triage and risk assessment in COVID-19 patients so that aggressive treatment strategies could be employed at the earliest to reduce mortalities due to COVID-19 in future.
Keywords: COVID-19; Nepal; mortality.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- WHO Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. [(accessed on 7 July 2021)]; Available online: https://covid19.who.int/
LinkOut - more resources
Full Text Sources
Miscellaneous
