

The use of augmented reality for limb and component alignment in total knee arthroplasty: systematic review of the literature and clinical pilot study
- PMID: 34287721
- PMCID: PMC8295423
- DOI: 10.1186/s40634-021-00374-7
The use of augmented reality for limb and component alignment in total knee arthroplasty: systematic review of the literature and clinical pilot study
Abstract
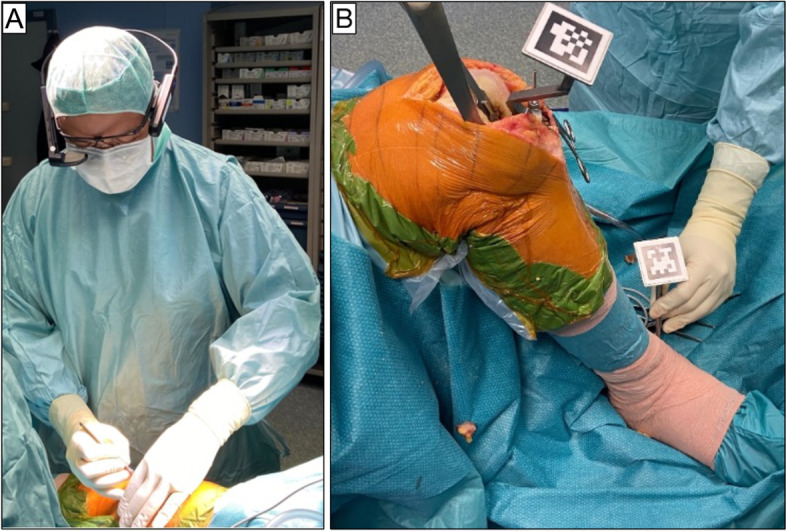
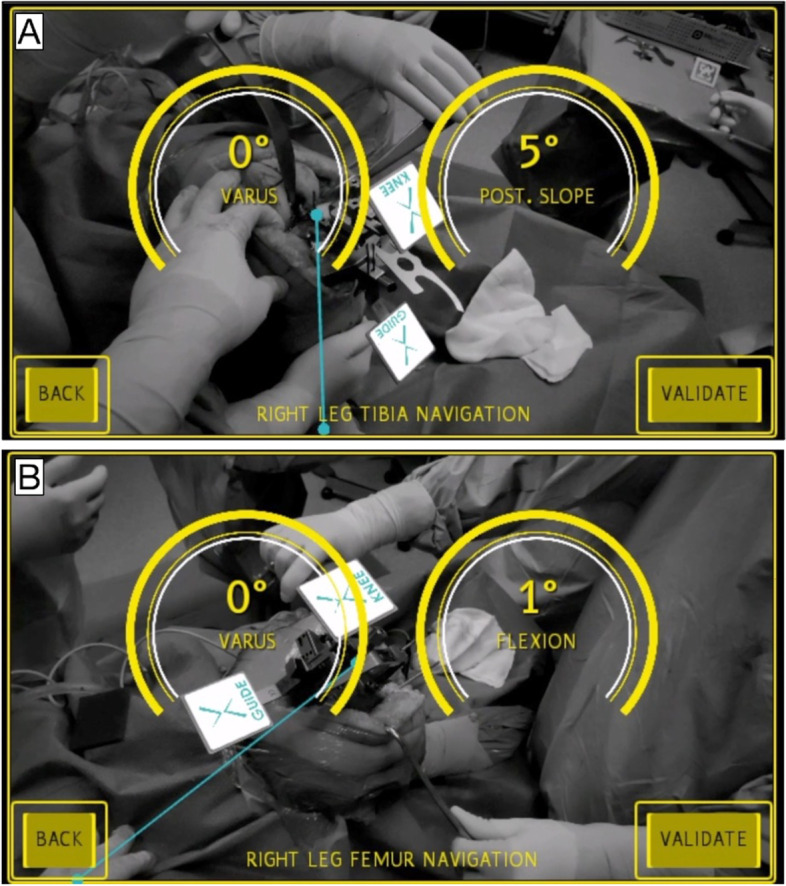
Purpose: A systematic review of the literature has been carried out to assess the actual evidence of the use of augmented reality in total knee arthroplasty (TKA). We then conducted a pilot clinical study to examine the accuracy of the Knee + augmented reality navigation in performing TKA. The present augmented reality (AR) system allows the surgeon to view the tibial and femur axis superimposed on the surgical field through the smart glasses. It provides real-time information during surgery and intraoperative feedback.
Methods: A systematic review of the PubMed, MEDLINE, and Embase databases up to May 2021 using the keywords "augmented reality", "knee arthroplasty", "computer assisted surgery", "navigation knee arthroplasty" was performed by two independent reviewers. We performed five TKAs using the Knee + system. Patients were 4 females, with mean age of 76.4 years old (range 73-79) and mean Body Max Index (BMI) of 31.9 kg/m2 (range 27-35). The axial alignment of the limb and the orientation of the components were evaluated on standardized pre and postoperative full leg length weight-bearing radiographs, anteroposterior radiographs, and lateral radiographs of the knee. The time of tourniquet was recorded. The perception of motion sickness was assessed by Virtual Reality Sickness Questionnaire (VRSQ) subjected to surgeon immediately after surgery.
Results: After duplicate removal, a total of 31 abstracts were found. However, only two studies concerned knee arthroplasty. Unfortunately, both were preclinical studies. Knee + system is able to perform a cutting error of less than 1° of difference about coronal alignment of femur and tibia and less than 2° about flexion/extension of femur and posterior tibial slope. The absolute differences between the values obtained during surgery and the measurement of varus femur, varus tibia, posterior slope, and femur flexion angle on post-operative radiographs were 0.6° ± 1.34°, 0.8° ± 0.84°, 0.8° ± 1.79°, and 0.4 mm ± 0.55 mm, respectively.
Conclusions: On light of our preliminary results, the Knee + system is accurate and effective to perform TKA. The translation from pilot study to high-level prospective studies is warranted to assess accuracy and cost-effective analysis compared to conventional techniques.
Level of evidence: IV.
Keywords: Augmented reality; Computer assisted surgery; Knee arthroplasty; Navigation knee arthroplasty.
© 2021. The Author(s).
Conflict of interest statement
Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Figures


Similar articles
-
Augmented reality-aided unicompartmental knee arthroplasty.J Exp Orthop. 2022 Sep 5;9(1):88. doi: 10.1186/s40634-022-00525-4. J Exp Orthop. 2022. PMID: 36064994 Free PMC article.
-
Single-center experience with Knee+™ augmented reality navigation system in primary total knee arthroplasty.World J Orthop. 2024 Mar 18;15(3):247-256. doi: 10.5312/wjo.v15.i3.247. eCollection 2024 Mar 18. World J Orthop. 2024. PMID: 38596188 Free PMC article.
-
Augmented reality-based navigation system applied to tibial bone resection in total knee arthroplasty.J Exp Orthop. 2019 Nov 11;6(1):44. doi: 10.1186/s40634-019-0212-6. J Exp Orthop. 2019. PMID: 31712907 Free PMC article.
-
Component placement accuracy in two generations of handheld robotics-assisted knee arthroplasty.Arch Orthop Trauma Surg. 2021 Dec;141(12):2059-2067. doi: 10.1007/s00402-021-04040-6. Epub 2021 Jul 25. Arch Orthop Trauma Surg. 2021. PMID: 34304279 Review.
-
Highly variable coronal tibial and femoral alignment in osteoarthritic knees: a systematic review.Knee Surg Sports Traumatol Arthrosc. 2019 May;27(5):1368-1377. doi: 10.1007/s00167-019-05506-2. Epub 2019 Apr 15. Knee Surg Sports Traumatol Arthrosc. 2019. PMID: 30989273
Cited by
-
The Accuracy and Absolute Reliability of a Knee Surgery Assistance System Based on ArUco-Type Sensors.Sensors (Basel). 2023 Sep 26;23(19):8091. doi: 10.3390/s23198091. Sensors (Basel). 2023. PMID: 37836921 Free PMC article.
-
A systematic literature review on integrating AI-powered smart glasses into digital health management for proactive healthcare solutions.NPJ Digit Med. 2025 Jul 5;8(1):410. doi: 10.1038/s41746-025-01715-x. NPJ Digit Med. 2025. PMID: 40617964 Free PMC article.
-
Total Knee Arthroplasty With Robotic and Augmented Reality Guidance: A Hierarchical Task Analysis.Arthroplast Today. 2024 Jun 27;27:101389. doi: 10.1016/j.artd.2024.101389. eCollection 2024 Jun. Arthroplast Today. 2024. PMID: 39071834 Free PMC article.
-
A pilot study on preferences from surgeons to deal with an innovative customized and connected knee prosthesis - A discret choice experiment.Heliyon. 2024 May 8;10(10):e30041. doi: 10.1016/j.heliyon.2024.e30041. eCollection 2024 May 30. Heliyon. 2024. PMID: 38784553 Free PMC article.
-
High accuracy and learning curve improvement of augmented reality in total knee arthroplasty: A single-centre study on 157 patients.J Exp Orthop. 2025 Jul 13;12(3):e70369. doi: 10.1002/jeo2.70369. eCollection 2025 Jul. J Exp Orthop. 2025. PMID: 40655245 Free PMC article.
References
-
- Casari FA, Navab N, Hruby LA, et al. Augmented Reality in Orthopedic Surgery Is Emerging from Proof of Concept Towards Clinical Studies: a Literature Review Explaining the Technology and Current State of the Art. Curr Rev Musculoskelet Med. 2021;14:192–203. doi: 10.1007/s12178-021-09699-3. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
