

Cerebroprotection for Acute Ischemic Stroke: Looking Ahead
- PMID: 34289710
- PMCID: PMC8384682
- DOI: 10.1161/STROKEAHA.121.032241
Cerebroprotection for Acute Ischemic Stroke: Looking Ahead
Abstract
We search for ischemic stroke treatment knowing we have failed-intensely and often-to translate mechanistic knowledge into treatments that alleviate our patients' functional impairments. Lessons can be derived from our shared failures that may point to new directions and new strategies. First, the principle criticisms of both preclinical and clinical assessments are summarized. Next, previous efforts to develop single-mechanism treatments are reviewed. Finally, new definitions, novel approaches, and different directions are presented. In previous development efforts, the basic science and preclinical assessment of candidate treatments often lacked rigor and sufficiency; the clinical trials may have lacked power, rigor, or rectitude; or most likely both preclinical and clinical investigations were flawed. Single-target agents directed against specific molecular mechanisms proved unsuccessful. The term neuroprotection should be replaced as it has become ambiguous: protection of the entire neurovascular unit may be called cerebral cytoprotection or cerebroprotection. Success in developing cerebroprotection-either as an adjunct to recanalization or as stand-alone treatment-will require new definitions that recognize the importance of differential vulnerability in the neurovascular unit. Recent focus on pleiotropic multi-target agents that act via multiple mechanisms of action to interrupt ischemia at multiple steps may be more fruitful. Examples of pleiotropic treatments include therapeutic hypothermia and 3K3A-APC (activated protein C). Alternatively, the single-target drug NA-1 triggers multiple downstream signaling events. Renewed commitment to scientific rigor is essential, and funding agencies and journals may enforce quality principles of rigor in preclinical science. Appropriate animal models should be selected that are suited to the purpose of the investigation. Before clinical trials, preclinical assessment could include subjects that are aged, of both sexes, and harbor comorbid conditions such as diabetes or hypertension. With these new definitions, novel approaches, and renewed attention to rigor, the prospect for successful cerebroprotective therapy should improve.
Keywords: clinical trial design; cytoprotection; hypertension; ischemia; review.
Figures
References
-
- Hort I, Karenberg A. Medieval descriptions and doctrines of stroke: Preliminary analysis of select sources. Part i: The struggle for terms and theories - late antiquity and early middle ages (300–800). Journal of the History of the Neurosciences. 1998;7:162–173 - PubMed
-
- Karenberg A, Hort I. Medieval descriptions and doctrines of stroke: Preliminary analysis of select sources. Part ii: Between galenism and aristotelism – islamic theories of apoplexy (800–1200). Journal of the History of the Neurosciences. 1998;7:174–185 - PubMed
-
- Astrup J, Siesjo BK, Symon L. Thresholds in cerebral ischemia: The ischemic penumbra. Stroke. 1981;12:723. - PubMed
-
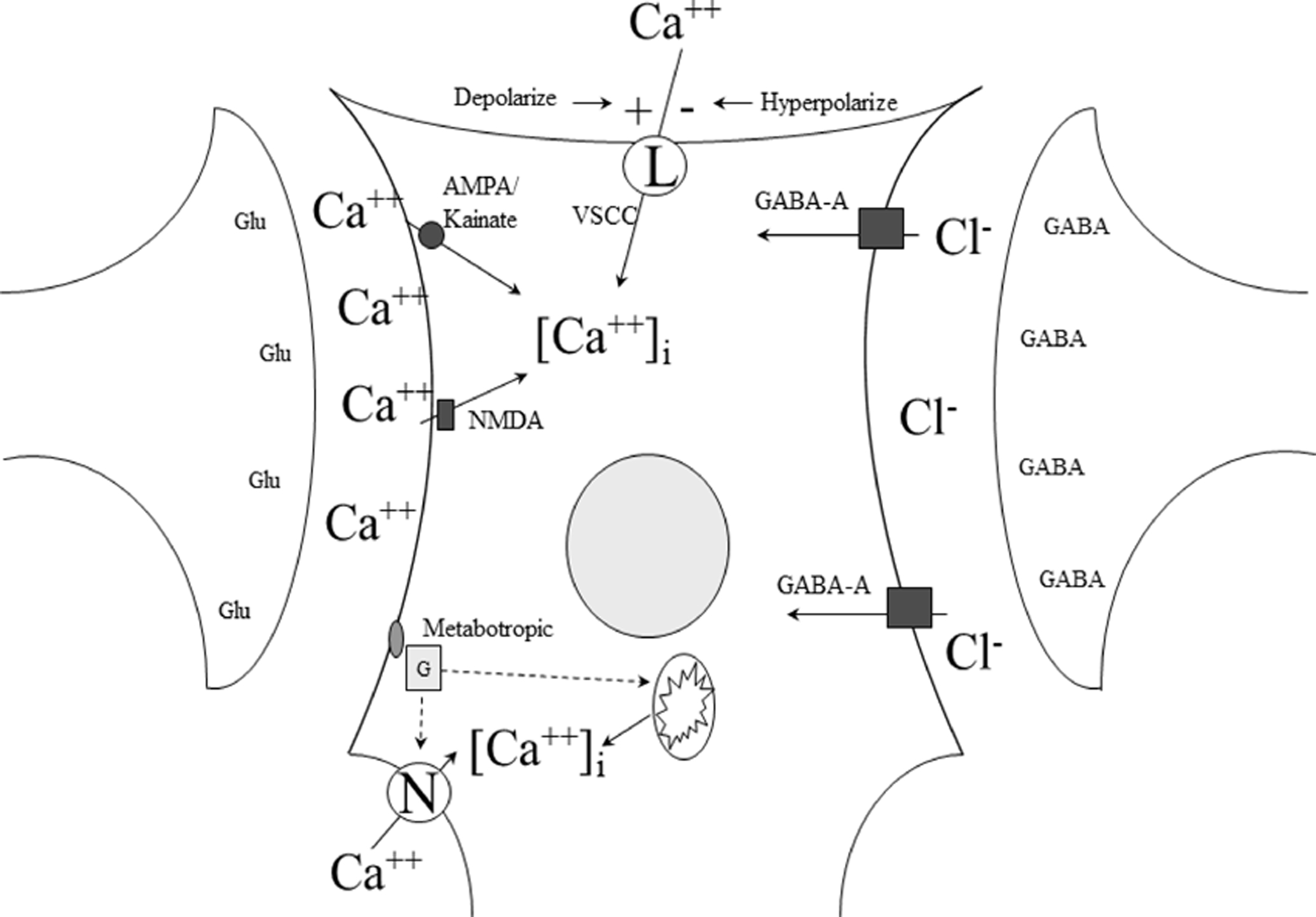
- Rothman SM, Olney JW. Excitotoxicity and the nmda receptor. Trends in Neuroscience. 1987;10:299 - PubMed
-
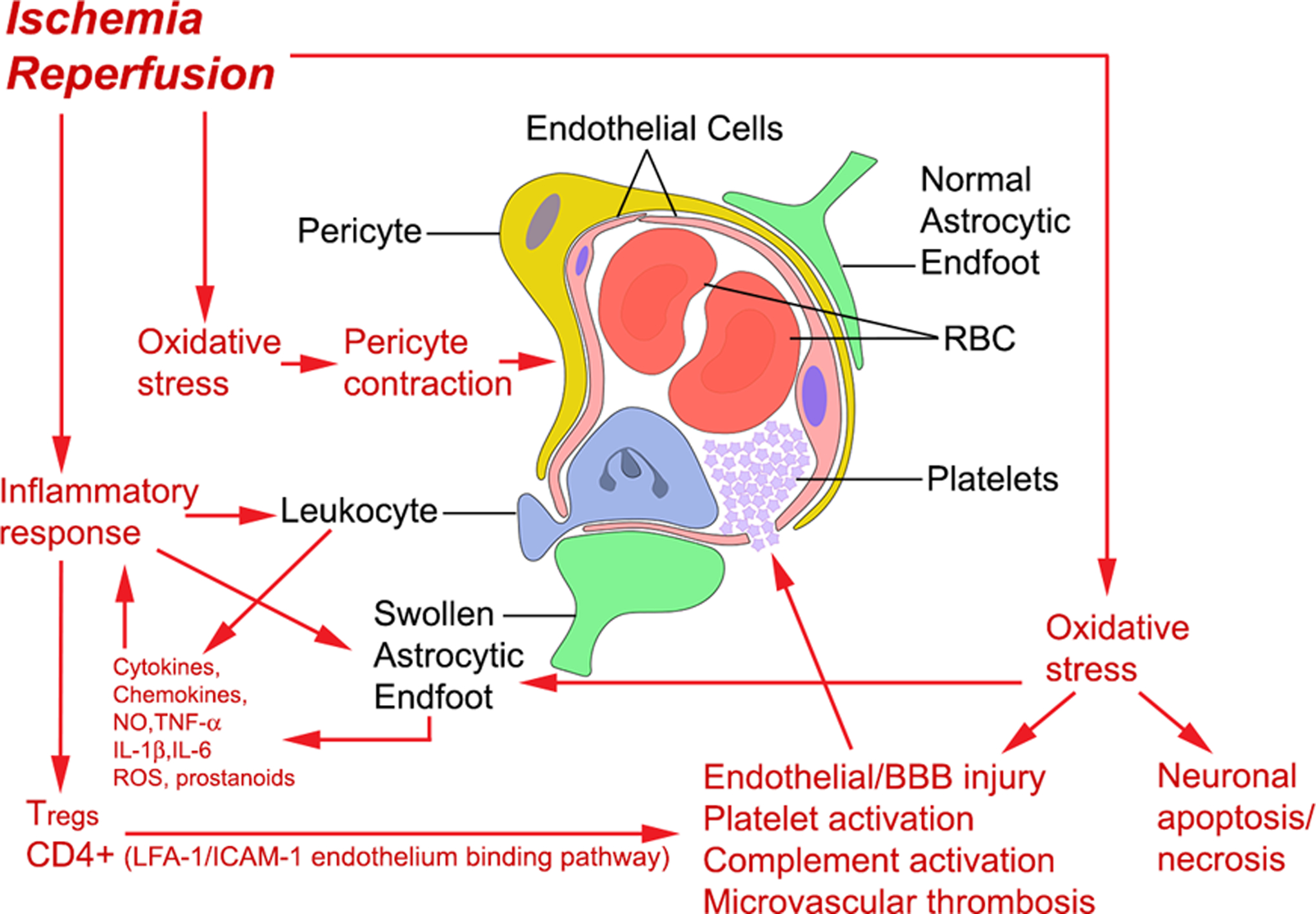
- Bai J, Lyden PD. Revisiting cerebral postischemic reperfusion injury: New insights in understanding reperfusion failure, hemorrhage, and edema. Int J Stroke. 2015;10:143–152 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
