

Treatment strategies for new onset atrial fibrillation in patients treated on an intensive care unit: a systematic scoping review
- PMID: 34289899
- PMCID: PMC8296751
- DOI: 10.1186/s13054-021-03684-5
Treatment strategies for new onset atrial fibrillation in patients treated on an intensive care unit: a systematic scoping review
Abstract
Background: New-onset atrial fibrillation (NOAF) in patients treated on an intensive care unit (ICU) is common and associated with significant morbidity and mortality. We undertook a systematic scoping review to summarise comparative evidence to inform NOAF management for patients admitted to ICU.
Methods: We searched MEDLINE, EMBASE, CINAHL, Web of Science, OpenGrey, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, Database of Abstracts of Reviews of Effects, ISRCTN, ClinicalTrials.gov, EU Clinical Trials register, additional WHO ICTRP trial databases, and NIHR Clinical Trials Gateway in March 2019. We included studies evaluating treatment or prevention strategies for NOAF or acute anticoagulation in general medical, surgical or mixed adult ICUs. We extracted study details, population characteristics, intervention and comparator(s), methods addressing confounding, results, and recommendations for future research onto study-specific forms.
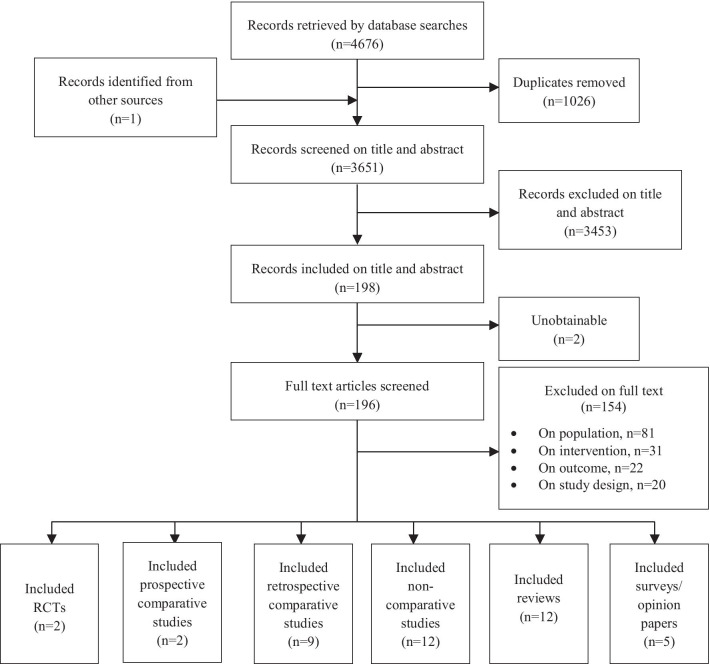
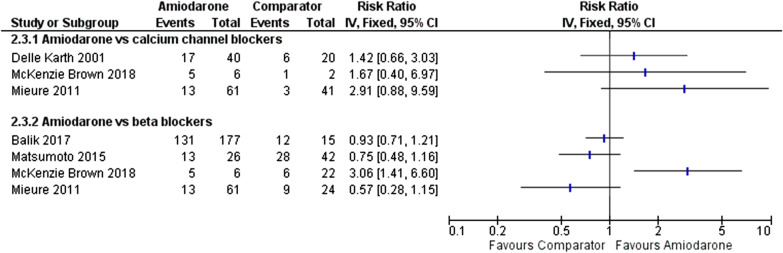
Results: Of 3,651 citations, 42 articles were eligible: 25 primary studies, 12 review articles and 5 surveys/opinion papers. Definitions of NOAF varied between NOAF lasting 30 s to NOAF lasting > 24 h. Only one comparative study investigated effects of anticoagulation. Evidence from small RCTs suggests calcium channel blockers (CCBs) result in slower rhythm control than beta blockers (1 study), and more cardiovascular instability than amiodarone (1 study). Evidence from 4 non-randomised studies suggests beta blocker and amiodarone therapy may be equivalent in respect to rhythm control. Beta blockers may be associated with improved survival compared to amiodarone, CCBs, and digoxin, though supporting evidence is subject to confounding. Currently, the limited evidence does not support therapeutic anticoagulation during ICU admission.
Conclusions: From the limited evidence available beta blockers or amiodarone may be superior to CCBs as first line therapy in undifferentiated patients in ICU. The little evidence available does not support therapeutic anticoagulation for NOAF whilst patients are critically ill. Consensus definitions for NOAF, rate and rhythm control are needed.
Keywords: Arrhythmia; Critical care; Intensive care; New onset atrial fibrillation; Scoping review; Stroke.
© 2021. The Author(s).
Conflict of interest statement
Paul Mouncey, Kathryn Rowan, and David Harrison have received grants from National Institute for Health Research. Peter Watkinson worked part time for Sensyne Health and has received grant funding from National Institute for Health Research, Wellcome, and Sensyne Health outside the submitted work. No other authors had competing interests to declare.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
