

Healthful and Unhealthful Plant-Based Diets and Risk of Breast Cancer in U.S. Women: Results from the Nurses' Health Studies
- PMID: 34289970
- PMCID: PMC8492491
- DOI: 10.1158/1055-9965.EPI-21-0352
Healthful and Unhealthful Plant-Based Diets and Risk of Breast Cancer in U.S. Women: Results from the Nurses' Health Studies
Abstract
Background: Plant-based diets have been associated with lower risk of various diseases, including type 2 diabetes, cardiovascular disease, and other cardiometabolic risk factors. However, the association between plant-based diet quality and breast cancer remains unclear.
Methods: We prospectively followed 76,690 women from the Nurses' Health Study (NHS, 1984-2016) and 93,295 women from the NHSII (1991-2017). Adherence to an overall plant-based diet index (PDI), a healthful PDI (hPDI), and an unhealthful PDI (uPDI) was assessed using previously developed indices. Cox proportional hazards models were used to estimate HR and 95% confidence intervals (CI) for incident invasive breast cancer.
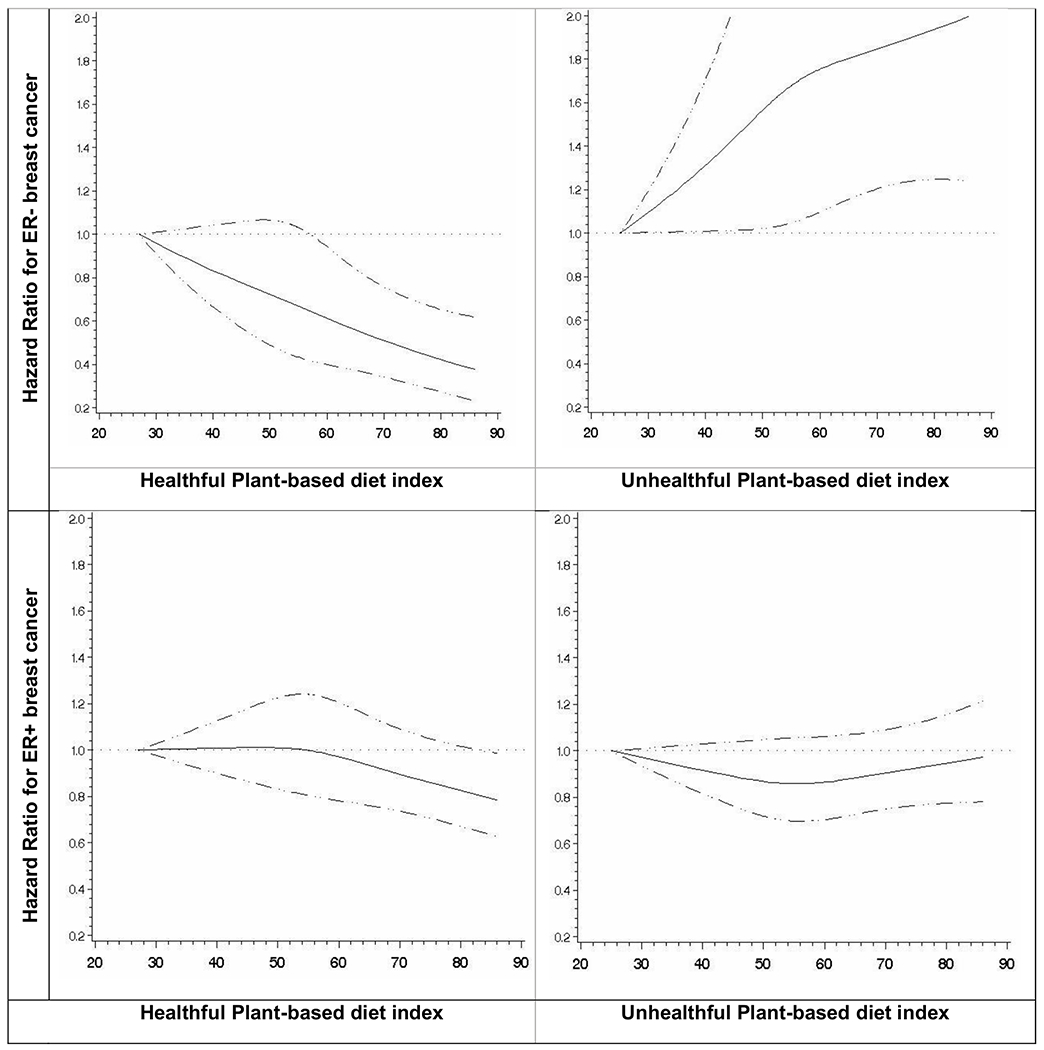
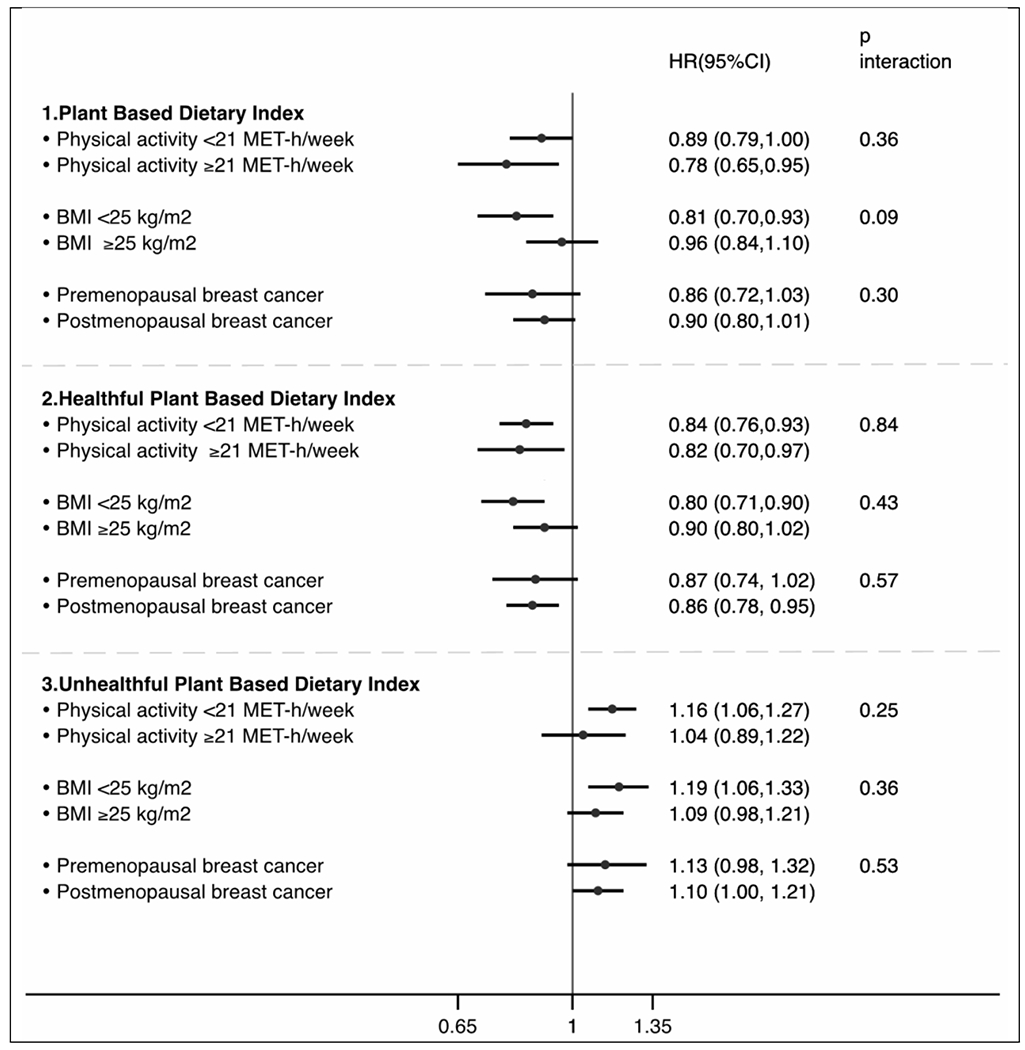
Results: Over 4,841,083 person-years of follow-up, we documented 12,482 incident invasive breast cancer cases. Women with greater adherence to PDI and hPDI were at modestly lower risk of breast cancer [(HRQ5 vs. Q1, 0.89; 95% CI, 0.84-0.95); (HRQ5 vs. Q1, 0.89; 95% CI, 0.83-0.94)]. We observed significant heterogeneity by estrogen receptor (ER) status, with the strongest inverse association between hPDI and breast cancer observed with ER-negative tumors [HRQ5 vs. Q1, 0.77; 95% CI, 0.65-0.90; P trend < 0.01]. We also found an inverse association between extreme quintiles of healthy plant foods and ER-negative breast cancer [HR, 0.74; 95% CI, 0.61-0.88; P trend < 0.01].
Conclusions: This study provides evidence that adherence to a healthful plant-based diet may reduce the risk of breast cancer, especially those that are more likely to be aggressive tumors.
Impact: This is the first prospective study investigating the relation between healthful and unhealthful plant-based dietary indices and risk of total and subtype-specific breast cancer.
©2021 American Association for Cancer Research.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
Similar articles
-
The quality of plant-based diets and liver cancer incidence and liver disease mortality in the UK Biobank.Clin Nutr ESPEN. 2025 Jun;67:541-548. doi: 10.1016/j.clnesp.2025.03.166. Epub 2025 Apr 3. Clin Nutr ESPEN. 2025. PMID: 40187730
-
Long-term adherence to healthful and unhealthful plant-based diets and breast cancer risk overall and by hormone receptor and histologic subtypes among postmenopausal females.Am J Clin Nutr. 2023 Mar;117(3):467-476. doi: 10.1016/j.ajcnut.2022.11.019. Am J Clin Nutr. 2023. PMID: 36872016 Free PMC article.
-
Plant-based diet quality and the risk of total and disease-specific mortality: A population-based prospective study.Clin Nutr. 2021 Dec;40(12):5718-5725. doi: 10.1016/j.clnu.2021.10.013. Epub 2021 Oct 25. Clin Nutr. 2021. PMID: 34749131
-
Scoping review of the association of plant-based diet quality with health outcomes.Front Nutr. 2023 Aug 10;10:1211535. doi: 10.3389/fnut.2023.1211535. eCollection 2023. Front Nutr. 2023. PMID: 37637943 Free PMC article.
-
The association between overall, healthy, and unhealthy plant-based diet indexes and risk of all-cause and cause-specific mortality: a systematic review and dose-response meta-analysis of prospective cohort studies.Food Funct. 2025 Mar 17;16(6):2194-2212. doi: 10.1039/d4fo04741a. Food Funct. 2025. PMID: 40018753
Cited by
-
Plant-based dietary patterns and the risk of digestive system cancers in 3 large prospective cohort studies.Eur J Epidemiol. 2023 Jun;38(6):617-627. doi: 10.1007/s10654-023-01007-2. Epub 2023 Apr 26. Eur J Epidemiol. 2023. PMID: 37101016
-
Dietary Interventions for Breast Cancer Prevention: Exploring the Role of Nutrition in Primary and Tertiary Prevention Strategies.Healthcare (Basel). 2025 Feb 13;13(4):407. doi: 10.3390/healthcare13040407. Healthcare (Basel). 2025. PMID: 39997282 Free PMC article. Review.
-
Plant-based dietary patterns and breast cancer risk in the European prospective investigation into cancer and nutrition (EPIC) study.Eur J Epidemiol. 2025 Aug;40(8):947-958. doi: 10.1007/s10654-025-01277-y. Epub 2025 Jul 14. Eur J Epidemiol. 2025. PMID: 40658296
-
Associations Between Dietary Factors and Breast Cancer Risk: A Systematic Review of Evidence from the MENA Region.Nutrients. 2025 Jan 22;17(3):394. doi: 10.3390/nu17030394. Nutrients. 2025. PMID: 39940252 Free PMC article.
-
Insulinemic potential of diet and risk of total and subtypes of breast cancer among US females.Am J Clin Nutr. 2022 Dec 19;116(6):1530-1539. doi: 10.1093/ajcn/nqac284. Am J Clin Nutr. 2022. PMID: 36178066 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
