

CT-derived 3D-diaphragm motion in emphysema and IPF compared to normal subjects
- PMID: 34290275
- PMCID: PMC8295260
- DOI: 10.1038/s41598-021-93980-5
CT-derived 3D-diaphragm motion in emphysema and IPF compared to normal subjects
Abstract
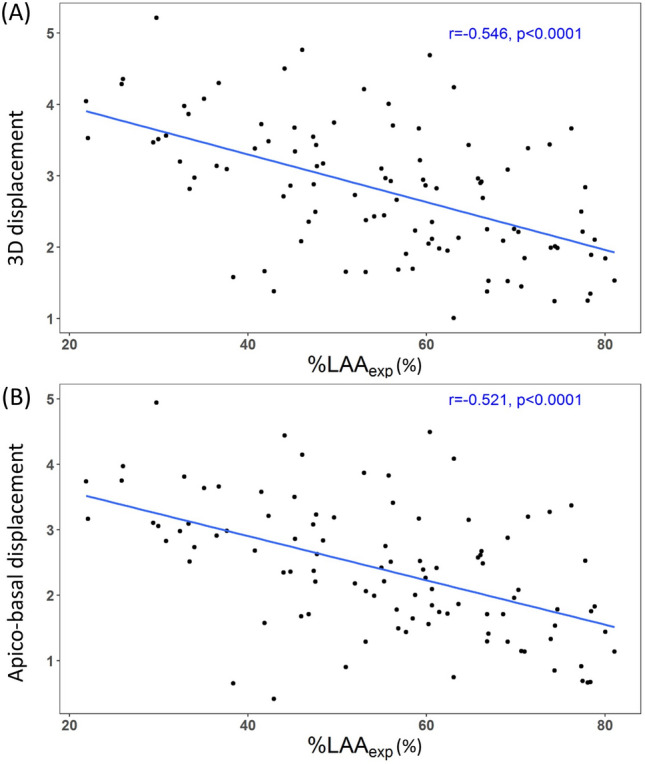
Image registration-based local displacement analysis enables evaluation of respiratory motion between two computed tomography-captured lung volumes. The objective of this study was to compare diaphragm movement among emphysema, idiopathic pulmonary fibrosis (IPF) and normal subjects. 29 normal, 50 emphysema, and 51 IPF subjects were included. A mass preserving image registration technique was used to compute displacement vectors of local lung regions at an acinar scale. Movement of the diaphragm was assumed to be equivalent to movement of the basal lung within 5 mm from the diaphragm. Magnitudes and directions of displacement vectors were compared between the groups. Three-dimensional (3D) and apico-basal displacements were smaller in emphysema than normal subjects (P = 0.003, P = 0.002). Low lung attenuation area on expiration scan showed significant correlations with decreased 3D and apico-basal displacements (r = - 0.546, P < 0.0001; r = - 0.521, P < 0.0001) in emphysema patients. Dorsal-ventral displacement was smaller in IPF than normal subjects (P < 0.0001). The standard deviation of the displacement angle was greater in both emphysema and IPF patients than normal subjects (P < 0.0001). In conclusion, apico-basal movement of the diaphragm is reduced in emphysema while dorsal-ventral movement is reduced in IPF. Image registration technique to multi-volume CT scans provides insight into the pathophysiology of limited diaphragmatic motion in emphysema and IPF.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures







References
-
- Davachi B, et al. The relationship between diaphragmatic movements in sonographic assessment and disease severity in patients with stable chronic obstructive pulmonary disease (COPD) J. Cardio-Thoracic Med. 2014;2:187–192.
