

AST to Platelet Ratio Index (APRI) is an easy-to-use predictor score for cardiovascular risk in metabolic subjects
- PMID: 34290320
- PMCID: PMC8295377
- DOI: 10.1038/s41598-021-94277-3
AST to Platelet Ratio Index (APRI) is an easy-to-use predictor score for cardiovascular risk in metabolic subjects
Abstract
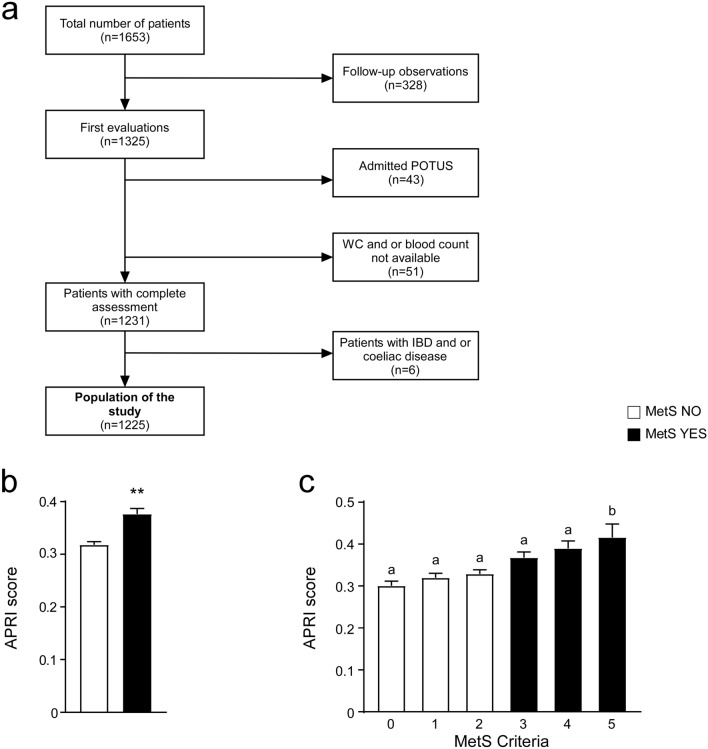
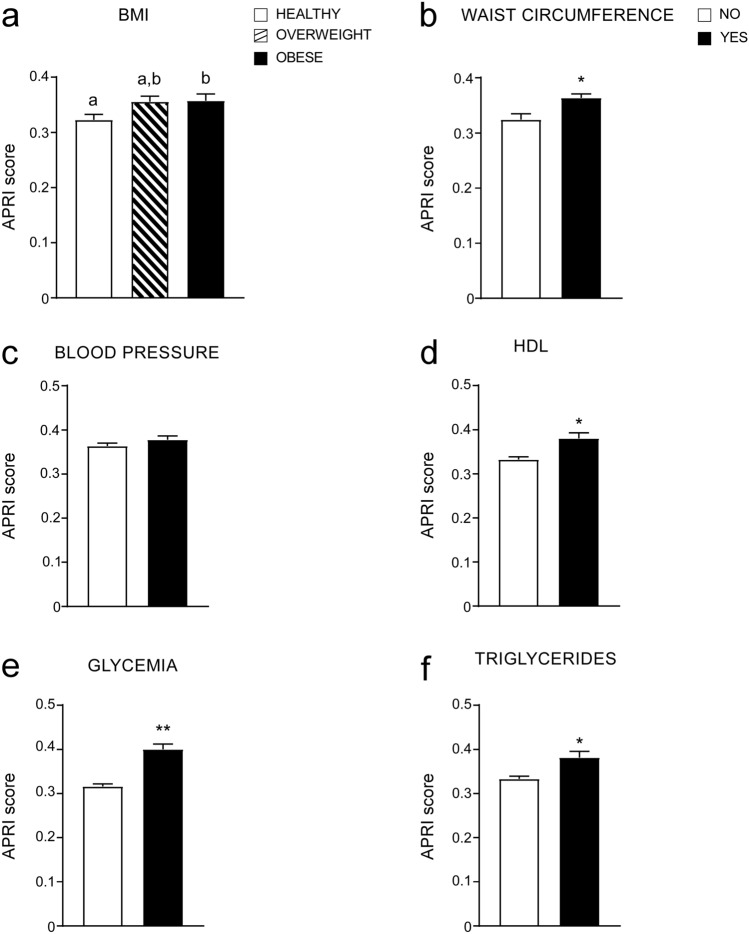
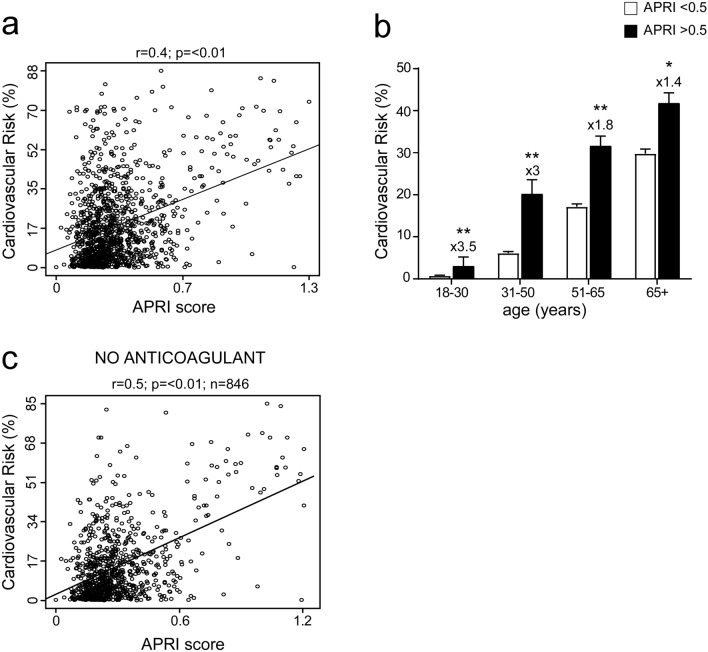
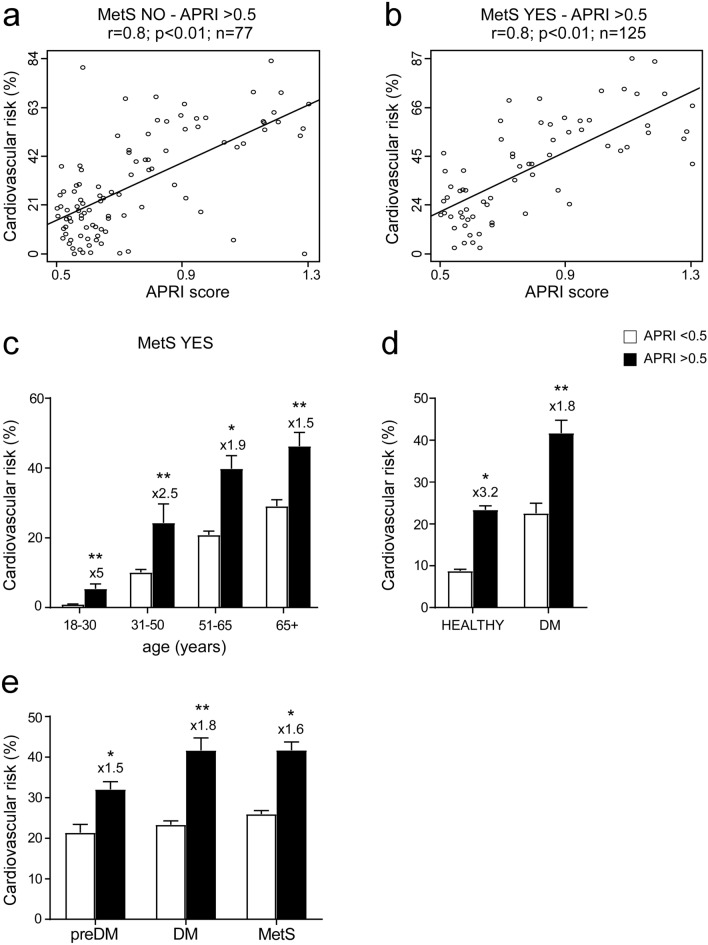
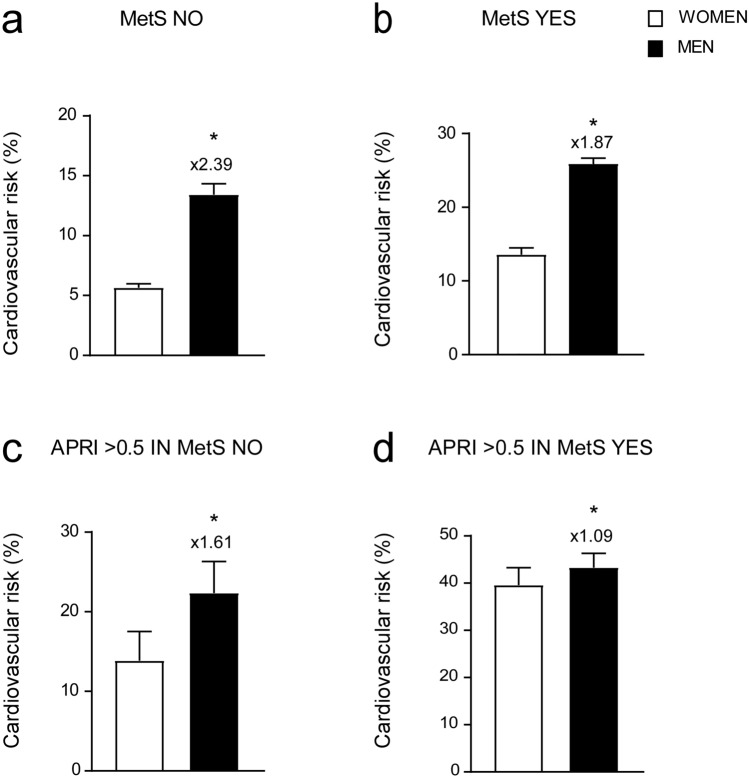
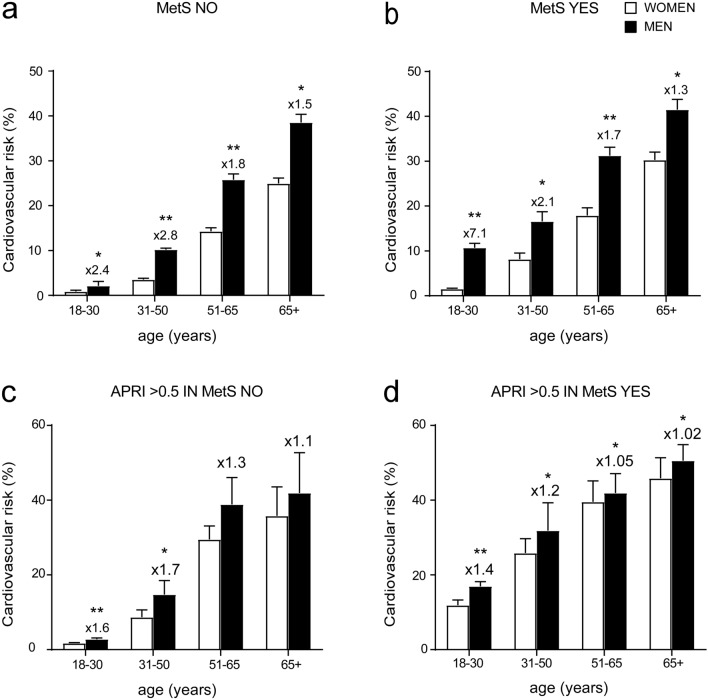
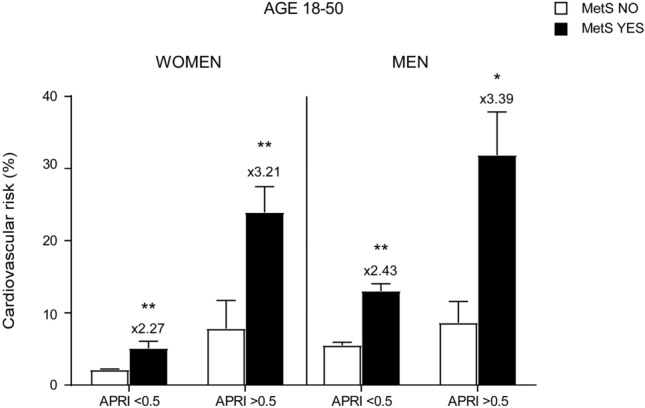
Visceral obesity is characterized by a low-grade inflammatory systemic state that contributes to the genesis of non-alcoholic fatty liver disease (NAFLD), frequently associated with liver fibrosis. Non-invasive serum markers have recently emerged as reliable, easy-to-use scores to predict liver fibrosis. NAFLD is often linked to metabolic and cardiovascular risk. Thus, in this cross-sectional study, we investigated in a population of 1225 subjects if AST to Platelet Ratio Index (APRI), one of the non-invasive liver fibrosis serum markers, can predict cardiovascular risk (CVR). APRI has been previously validated as an efficient score to predict liver fibrosis in viral hepatitis patients with a cut-off of 0.5 for fibrosis and 1.5 for cirrhosis. Our study showed that APRI significantly correlates with CVR and determines, when elevated, a significant increase in CVR for both genders, especially females. This spike in CVR, observed when APRI is elevated, is relatively high in patients in the age of 51-65 years, but it is significantly higher in younger and premenopausal women, approaching risk values usually typical of men at the same age. Taken together, our data highlighted the role of APRI as a reliable predictor easy-to-use score for CVR in metabolic patients.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
