

Sensory Stimulation of the Foot and Ankle Early Post-stroke: A Pilot and Feasibility Study
- PMID: 34290663
- PMCID: PMC8287025
- DOI: 10.3389/fneur.2021.675106
Sensory Stimulation of the Foot and Ankle Early Post-stroke: A Pilot and Feasibility Study
Abstract
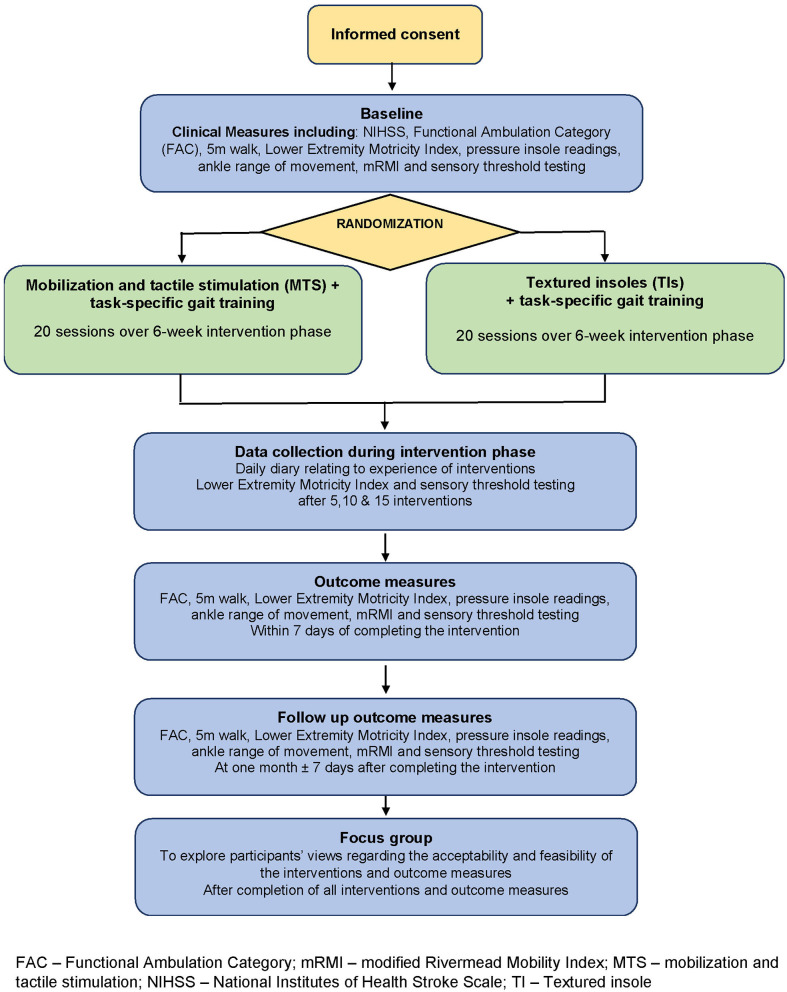
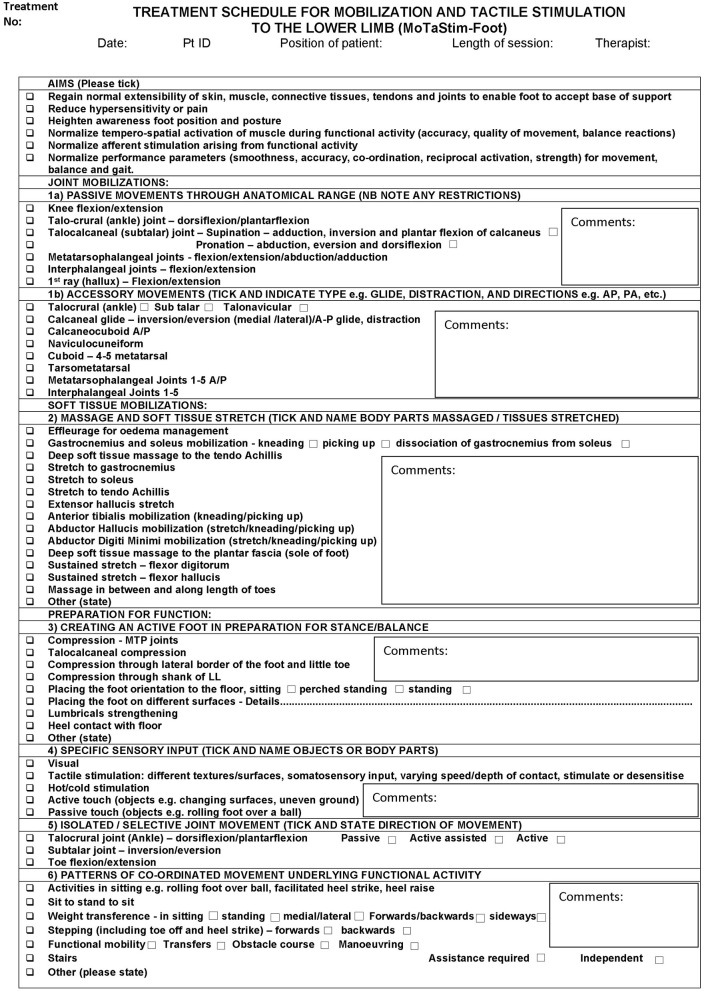
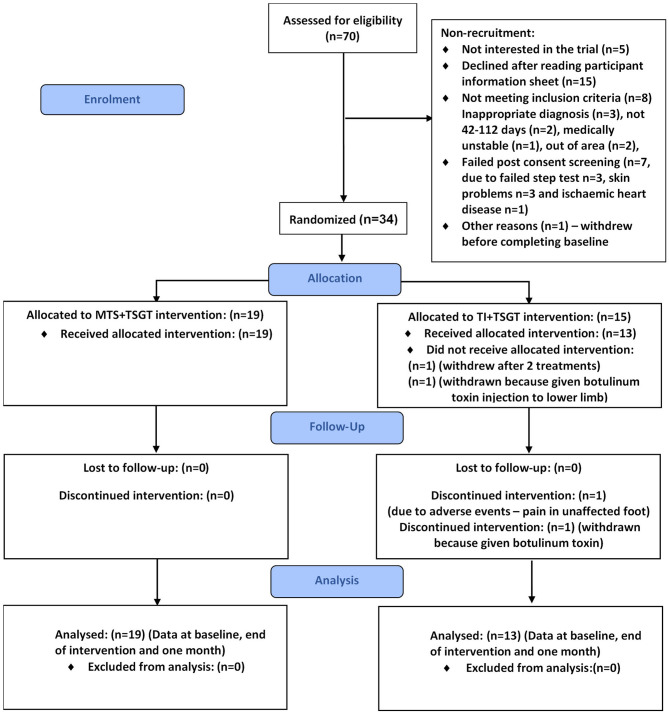
Background: Somatosensory stimulation of the lower extremity could improve motor recovery and walking post-stroke. This pilot study investigated the feasibility of a subsequent randomized controlled trial (RCT) to determine whether task-specific gait training is more effective following either (a) intensive hands-on somatosensory stimulation or (b) wearing textured insoles. Objectives: Determine recruitment and attrition rates, adherence to intervention, acceptability and viability of interventions and outcome measures, and estimate variance of outcome data to inform sample size for a subsequent RCT. Methods: Design: randomized, single-blinded, mixed-methods pilot study. Setting: In-patient rehabilitation ward and community. Participants: n = 34, 18+years, 42-112 days following anterior or posterior circulation stroke, able to follow simple commands, able to walk independently pre-stroke, and providing informed consent. Intervention: Twenty 30-min sessions of task-specific gait training (TSGT) (delivered over 6 weeks) in addition to either: (a) 30-60 min mobilization and tactile stimulation (MTS); or (b) unlimited textured insole (TI) wearing. Outcomes: Ankle range of movement (electrogoniometer), touch-pressure sensory thresholds (Semmes Weinstein Monofilaments), motor impairment (Lower Extremity Motricity Index), walking ability and speed (Functional Ambulation Category, 5-m walk test, pressure insoles) and function (modified Rivermead Mobility Index), measured before randomization, post-intervention, and 1-month thereafter (follow-up). Adherence to allocated intervention and actual dose delivered (fidelity) were documented in case report forms and daily diaries. Focus groups further explored acceptability of interventions and study experience. Analysis: Recruitment, attrition, and dose adherence rates were calculated as percentages of possible totals. Thematic analysis of daily diaries and focus group data was undertaken. Standard deviations of outcome measures were calculated and used to inform a sample size calculation. Results: Recruitment, attrition, and adherence rates were 48.57, 5.88, and 96.88%, respectively. Focus groups, daily-diaries and case report forms indicated acceptability of interventions and outcome measures to participants. The 5-m walk was selected as primary outcome measure for a future trial [mean (SD) at end of intervention: 16.86 (11.24) MTS group and 21.56 (13.57) TI group]; sample size calculation indicated 60 participants are required per group. Conclusion: Recruitment, attrition and adherence rates and acceptability of interventions and outcomes justify a subsequent powered RCT of MTS+TSGT compared with TI+TSGT.
Keywords: feasibility study; lower extremity; motor recovery; rehabilitation; sensory retraining; somatosensory stimulation; stroke.
Copyright © 2021 Aries, Pomeroy, Sim, Read and Hunter.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Stroke-Association . State of the Nation - Stroke Statistics. Stroke Association (2017). Available online at: https://www.stroke.org.uk/sites/default/files/state_of_the_nation_2017_f...; https://www.stroke.org.uk/resources/state-nation-stroke-statistics?gclid...
-
- Feigenson JS, McCarthy ML, Meese PD, Feigenson WD, Greenberg SD, Rubin E, et al. . Stroke rehabilitation I. Factors predicting outcome and length of stay-an overview. N Y State J Med. (1977) 77:1426–30. - PubMed
-
- Carey LM. Stroke Rehabilitation Insights From Neuroscience and Imaging. Oxford: Oxford University Press; (2012).
LinkOut - more resources
Full Text Sources