

Early Prediction of Mortality, Severity, and Length of Stay in the Intensive Care Unit of Sepsis Patients Based on Sepsis 3.0 by Machine Learning Models
- PMID: 34291058
- PMCID: PMC8288021
- DOI: 10.3389/fmed.2021.664966
Early Prediction of Mortality, Severity, and Length of Stay in the Intensive Care Unit of Sepsis Patients Based on Sepsis 3.0 by Machine Learning Models
Abstract
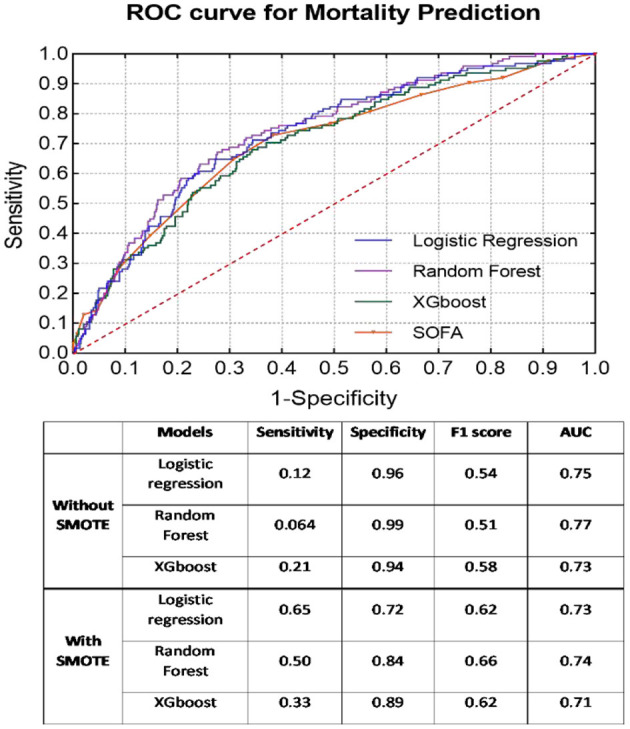
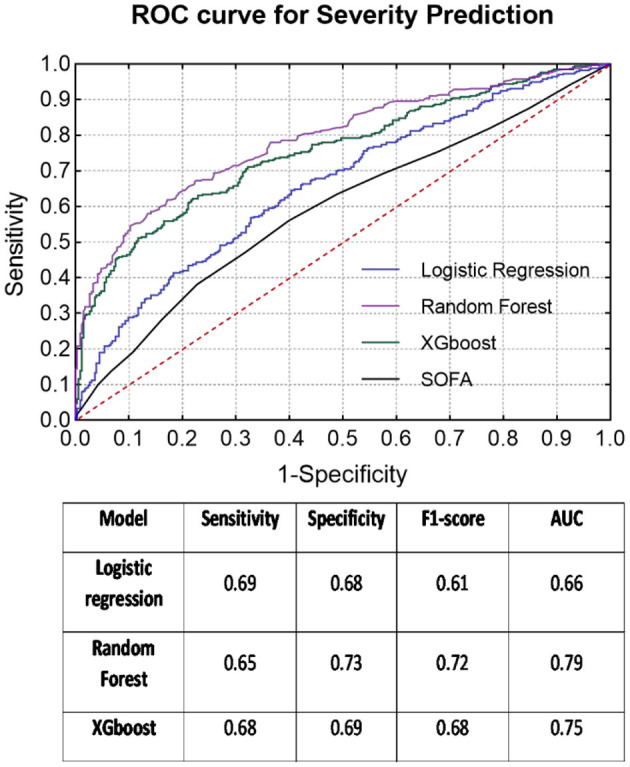
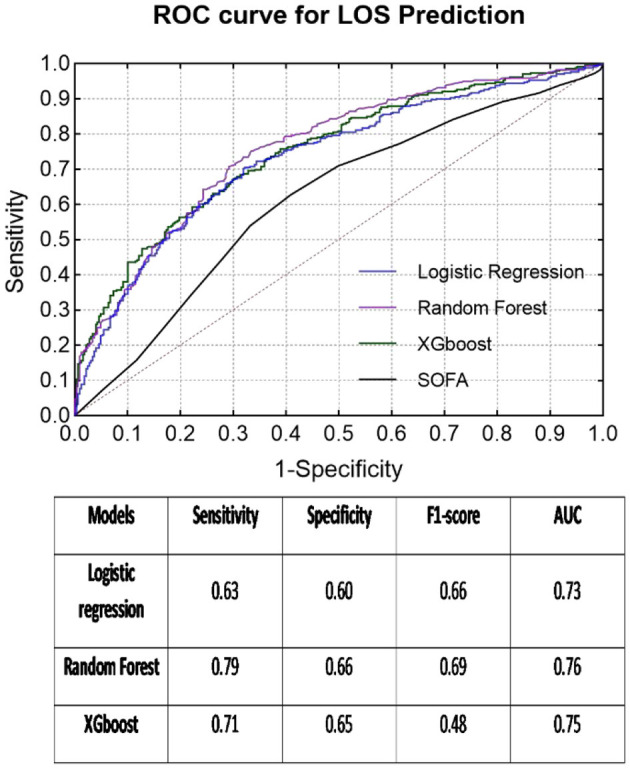
Background: Early prediction of the clinical outcome of patients with sepsis is of great significance and can guide treatment and reduce the mortality of patients. However, it is clinically difficult for clinicians. Methods: A total of 2,224 patients with sepsis were involved over a 3-year period (2016-2018) in the intensive care unit (ICU) of Peking Union Medical College Hospital. With all the key medical data from the first 6 h in the ICU, three machine learning models, logistic regression, random forest, and XGBoost, were used to predict mortality, severity (sepsis/septic shock), and length of ICU stay (LOS) (>6 days, ≤ 6 days). Missing data imputation and oversampling were completed on the dataset before introduction into the models. Results: Compared to the mortality and LOS predictions, the severity prediction achieved the best classification results, based on the area under the operating receiver characteristics (AUC), with the random forest classifier (sensitivity = 0.65, specificity = 0.73, F1 score = 0.72, AUC = 0.79). The random forest model also showed the best overall performance (mortality prediction: sensitivity = 0.50, specificity = 0.84, F1 score = 0.66, AUC = 0.74; LOS prediction: sensitivity = 0.79, specificity = 0.66, F1 score = 0.69, AUC = 0.76) among the three models. The predictive ability of the SOFA score itself was inferior to that of the above three models. Conclusions: Using the random forest classifier in the first 6 h of ICU admission can provide a comprehensive early warning of sepsis, which will contribute to the formulation and management of clinical decisions and the allocation and management of resources.
Keywords: machine learning; outcome; prediction; sepsis; sequential (sepsis-related) organ failure assessment.
Copyright © 2021 Su, Xu, Chang, Ma, Liu, Jiang, Wang, Li, Chen, Zhou, Hong, Zhu and Long.
Conflict of interest statement
ZX, FC, YM, and NH were employed by the DHC Software Co. Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Vincent JL, Moreno R, Takala J, Willatts S, De Mendonca A, Bruining H, et al. The SOFA (sepsis-related organ failure assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. (1996) 22:707–10. 10.1007/BF01709751 - DOI - PubMed
-
- Vincent JL, de Mendonca A, Cantraine F, Moreno R, Takala J, Suter PM, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit Care Med. (1998) 26:1793–800. 10.1097/00003246-199811000-00016 - DOI - PubMed
LinkOut - more resources
Full Text Sources