

Hospital variation in sphincter-preservation rates in rectal cancer treatment: results of a population-based study in the Netherlands
- PMID: 34291288
- PMCID: PMC8295312
- DOI: 10.1093/bjsopen/zrab065
Hospital variation in sphincter-preservation rates in rectal cancer treatment: results of a population-based study in the Netherlands
Abstract
Background: This study aimed to examine the sphincter-preservation rate variations in rectal cancer surgery. The influence of hospital volume on sphincter-preservation rates and short-term outcomes (anastomotic leakage (AL), positive circumferential resection margin (CRM), 30- and 90-day mortality rates) were also analysed.
Methods: Non-metastasized rectal cancer patients treated between 2009 and 2016 were selected from the Netherlands Cancer Registry. Surgical procedures were divided into sphincter-preserving surgery and an end colostomy group. Multivariable logistic regression models were generated to estimate the probability of undergoing sphincter-preserving surgery according to the hospital of surgery and tumour height (low, 5 cm or less, mid, more than 5 cm to 10 cm, and high, more than 10 cm). The influence of annual hospital volume (less than 20, 20-39, more than 40 resections) on sphincter-preservation rate and short-term outcomes was also examined.
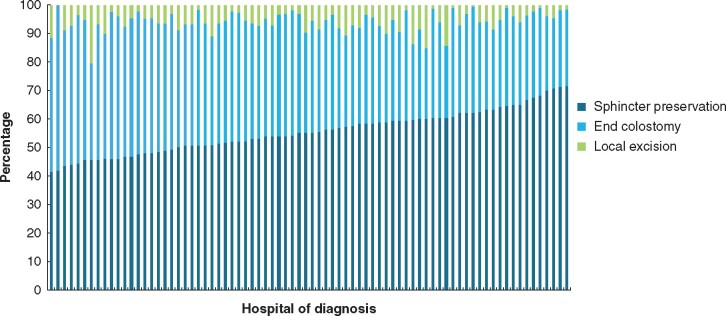
Results: A total of 20 959 patients were included (11 611 sphincter preservation and 8079 end colostomy) and the observed median sphincter-preservation rate in low, mid and high rectal cancer was 29.3, 75.6 and 87.9 per cent respectively. After case-mix adjustment, hospital of surgery was a significant factor for patients' likelihood for sphincter preservation in all three subgroups (P < 0.001). In mid rectal cancer, borderline higher rates of sphincter preservation were associated with low-volume hospitals (odds ratio 1.20, 95 per cent c.i. 1.01 to 1.43). No significant association between annual hospital volume and sphincter-preservation rate in low and high rectal cancer nor short-term outcomes (AL, positive CRM rate and 30- and 90-day mortality rates) was identified.
Conclusion: This population-based study showed a significant hospital variation in sphincter-preservation rates in rectal surgery. The annual hospital volume, however, was not associated with sphincter-preservation rates in low, and high rectal cancer nor with other short-term outcomes.
© The Author(s) 2021. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures



Similar articles
-
The Influence of Hospital Volume on Circumferential Resection Margin Involvement: Results of the Dutch Surgical Colorectal Audit.Ann Surg. 2016 Apr;263(4):745-50. doi: 10.1097/SLA.0000000000001009. Ann Surg. 2016. PMID: 25790120
-
Population-based use of sphincter-preserving surgery in patients with rectal cancer: is there room for improvement?Dis Colon Rectum. 2013 Jun;56(6):704-10. doi: 10.1097/DCR.0b013e3182758c2b. Dis Colon Rectum. 2013. PMID: 23652743
-
No difference between lowest and highest volume hospitals in outcome after colorectal cancer surgery in the southern Netherlands.Eur J Surg Oncol. 2013 Nov;39(11):1199-206. doi: 10.1016/j.ejso.2013.08.020. Epub 2013 Sep 3. Eur J Surg Oncol. 2013. PMID: 24044806
-
Sphincter-preserving operations for rectal cancer.Oncology (Williston Park). 1996 Nov;10(11):1673-84, 1689; discussion 1690-2. Oncology (Williston Park). 1996. PMID: 8953588 Review.
-
Methods and results of sphincter-preserving surgery for rectal cancer.Cancer Control. 2003 May-Jun;10(3):212-8. doi: 10.1177/107327480301000304. Cancer Control. 2003. PMID: 12794619 Review.
Cited by
-
Preferences for treatment outcomes in rectal cancer: A discrete choice experiment among patients and healthy volunteers.Colorectal Dis. 2025 Feb;27(2):e70021. doi: 10.1111/codi.70021. Colorectal Dis. 2025. PMID: 39924856 Free PMC article.
-
Optimization of rectal cancer surgery outcomes in the United States: the influence of hospital volume on rates of sphincter preservation before and after practice standardization.Proc (Bayl Univ Med Cent). 2025 May 27;38(4):375-386. doi: 10.1080/08998280.2025.2503653. eCollection 2025. Proc (Bayl Univ Med Cent). 2025. PMID: 40557207 Free PMC article.
-
Socio-economic predictors and between-hospital variation in permanent stoma rates after segmental resection of colorectal cancer. A population-based register study.Colorectal Dis. 2025 Jul;27(7):e70153. doi: 10.1111/codi.70153. Colorectal Dis. 2025. PMID: 40635412 Free PMC article.
-
Patterns of Care and Outcomes of Rectal Cancer Patients from the Iowa Cancer Registry: Role of Hospital Volume and Tumor Location.J Gastrointest Surg. 2023 Jun;27(6):1228-1237. doi: 10.1007/s11605-023-05656-2. Epub 2023 Mar 22. J Gastrointest Surg. 2023. PMID: 36949239 Free PMC article.
References
-
- Weitz J, Koch M, Debus J, Hohler T, Galle PR, Buchler MW. Colorectal cancer. Lancet 2005;365:153–165 - PubMed
-
- Jonker FHW, Hagemans JAW, Burger JWA, Verhoef C, Borstlap WAA, Tanis PJ; Dutch Snapshot Research Group. The influence of hospital volume on long-term oncological outcome after rectal cancer surgery. Int J Colorectal Dis 2017;32:1741–1747 - PubMed
-
- Harling H, Bulow S, Moller LN, Jorgensen T; the Danish Colorectal Cancer Groups. Hospital volume and outcome of rectal cancer surgery in Denmark 1994–99. Colorectal Dis 2005;7:90–95 - PubMed
-
- Meyerhardt JA, Tepper JE, Niedzwiecki D, Hollis DR, Schrag D, Ayanian JZ et al. Impact of hospital procedure volume on surgical operation and long-term outcomes in high-risk curatively resected rectal cancer: findings from the Intergroup 0114 Study. J Clin Oncol 2004;22:166–174 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
