

Endoscopic third ventriculostomy before surgery of third ventricle and posterior fossa tumours decreases the risk of secondary hydrocephalus and early postoperative complications
- PMID: 34291350
- PMCID: PMC8827142
- DOI: 10.1007/s10143-021-01570-w
Endoscopic third ventriculostomy before surgery of third ventricle and posterior fossa tumours decreases the risk of secondary hydrocephalus and early postoperative complications
Abstract
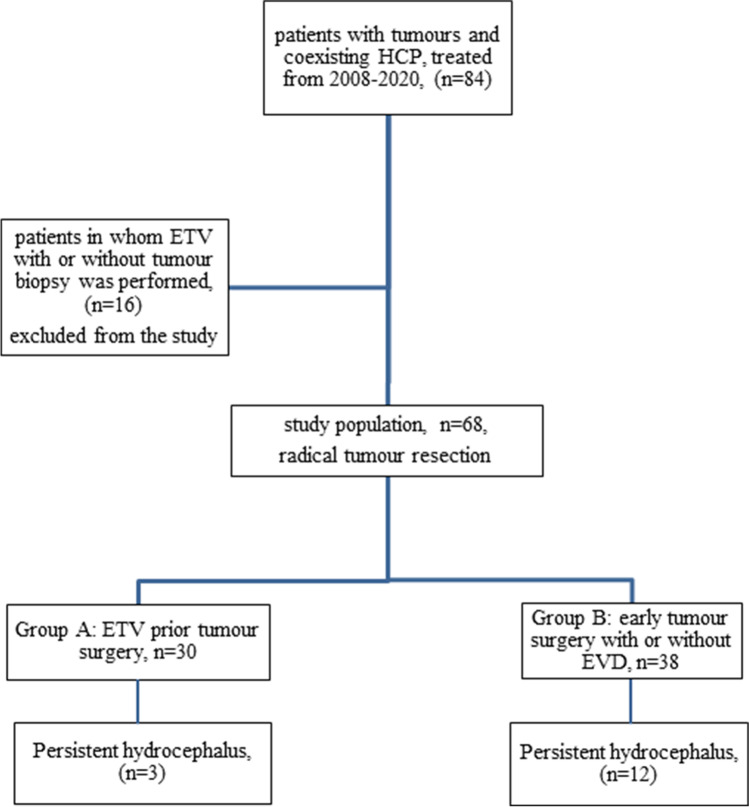
Endoscopic third ventriculostomy (ETV) is an effective treatment for obstructive hydrocephalus (HCP) at the level of third or fourth ventricle. To date, there is no consensus regarding its role as intervention preceding the operation of tumour removal. The aim of this prospective open-label controlled study is to assess if ETV prevents secondary HCP after tumour removal and if ETV influences the early results of tumour surgery. The study was performed on 68 patients operated for tumours of the third ventricle and posterior fossa. In 30 patients, ETV was performed several days before tumour removal, while in 38 patients, the tumour was removed during a one-stage procedure without ETV. Patients who did not receive ETV before the tumour removal procedure had a higher probability of developing postoperative HCP (n = 12, p = 0.03). They also demonstrated a substantially higher rate of early postoperative complications (n = 20, p = 0.002) and a lower Karnofsky score (p = 0.004) than patients in whom ETV was performed before tumour removal. The performance of external ventricular drainage in the non-ETV group did not prevent secondary HCP (p = 0.68). Postoperative cerebellar swelling (p = 0.01), haematoma (p = 0.04), cerebrospinal fluid leak (p = 0.04) and neuroinfection (p = 0.04) were the main risk factors of persistent HCP. Performance of ETV before tumour removal is not only beneficial for control of acute HCP but also prevents the occurrence of secondary postoperative HCP and may also minimize early postoperative complications.
Keywords: Endoscopic third ventriculostomy; Secondary postoperative hydrocephalus; Tumour removal.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Di Rocco F, Jucá CE, Zerah M, Sainte-Rose C (2013) Endoscopic third ventriculostomy and posterior fossa tumors. World Neurosurg 79(2 Suppl): S18.e15–9 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
