

US Trends in Opioid Access Among Patients With Poor Prognosis Cancer Near the End-of-Life
- PMID: 34292766
- PMCID: PMC8425843
- DOI: 10.1200/JCO.21.00476
US Trends in Opioid Access Among Patients With Poor Prognosis Cancer Near the End-of-Life
Abstract
Purpose: Heightened regulations have decreased opioid prescribing across the United States, yet little is known about trends in opioid access among patients dying of cancer.
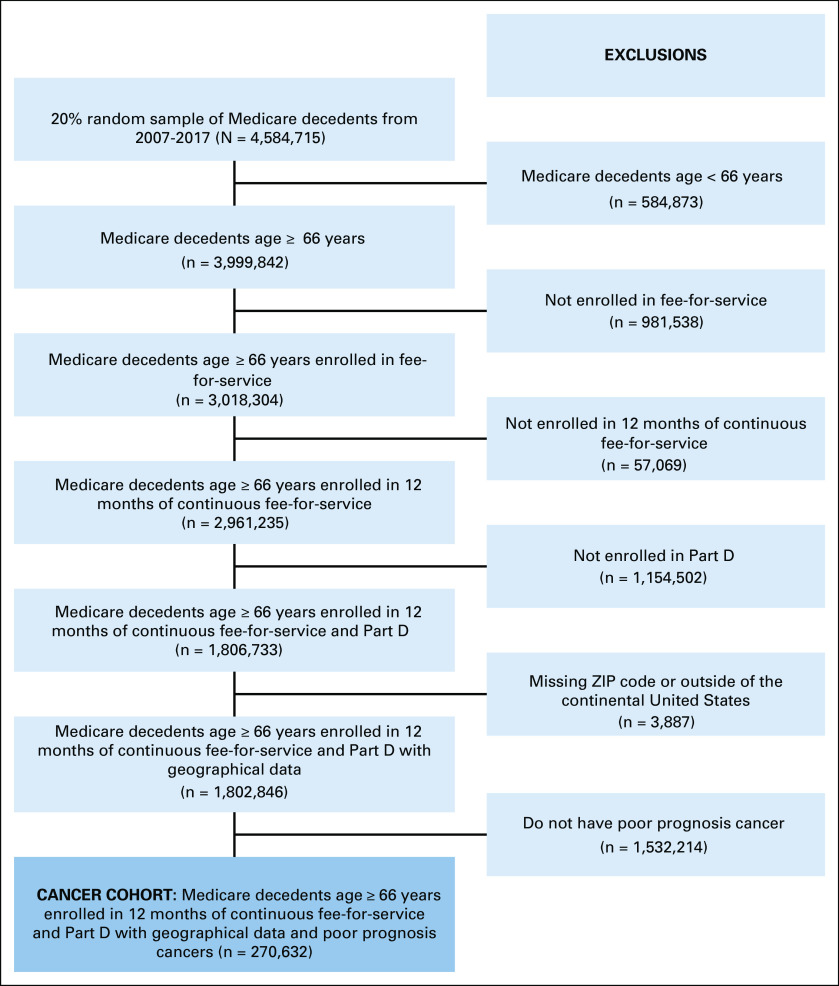
Methods: Among 270,632 Medicare fee-for-service decedents with poor prognosis cancers, we used part D data to examine trends from 2007 to 2017 in opioid prescription fills and opioid potency (morphine milligram equivalents per day [MMED]) near the end-of-life (EOL), defined as the 30 days before death or hospice enrollment. We used administrative claims to evaluate trends in pain-related emergency department (ED) visits near EOL.
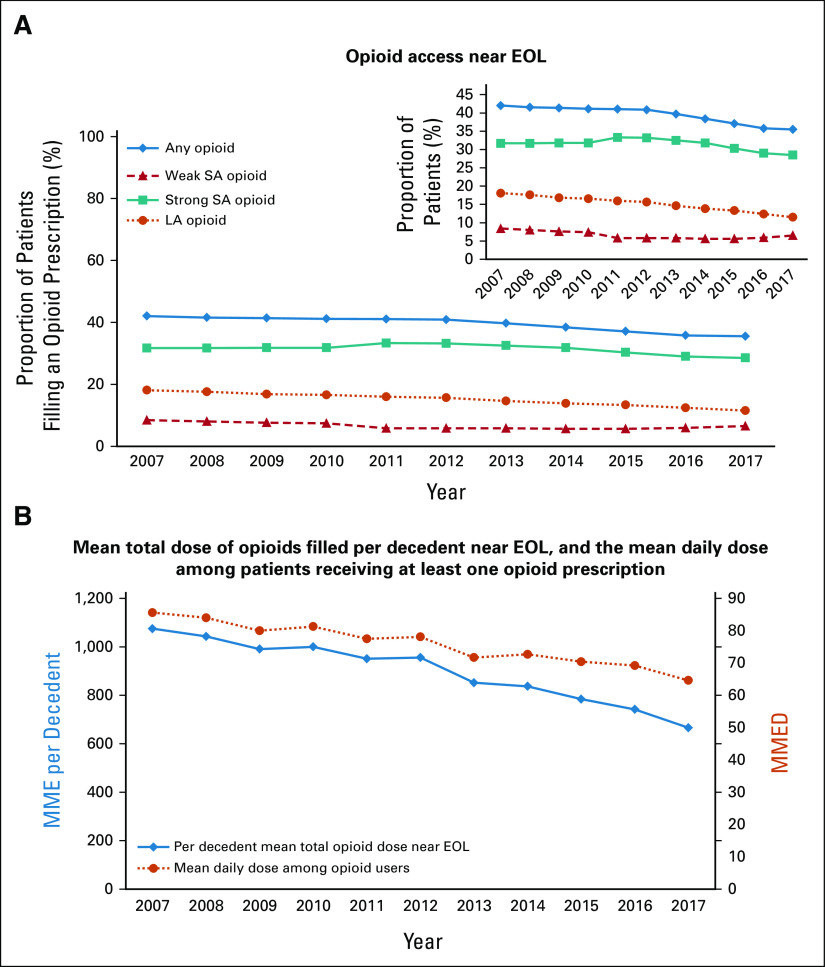
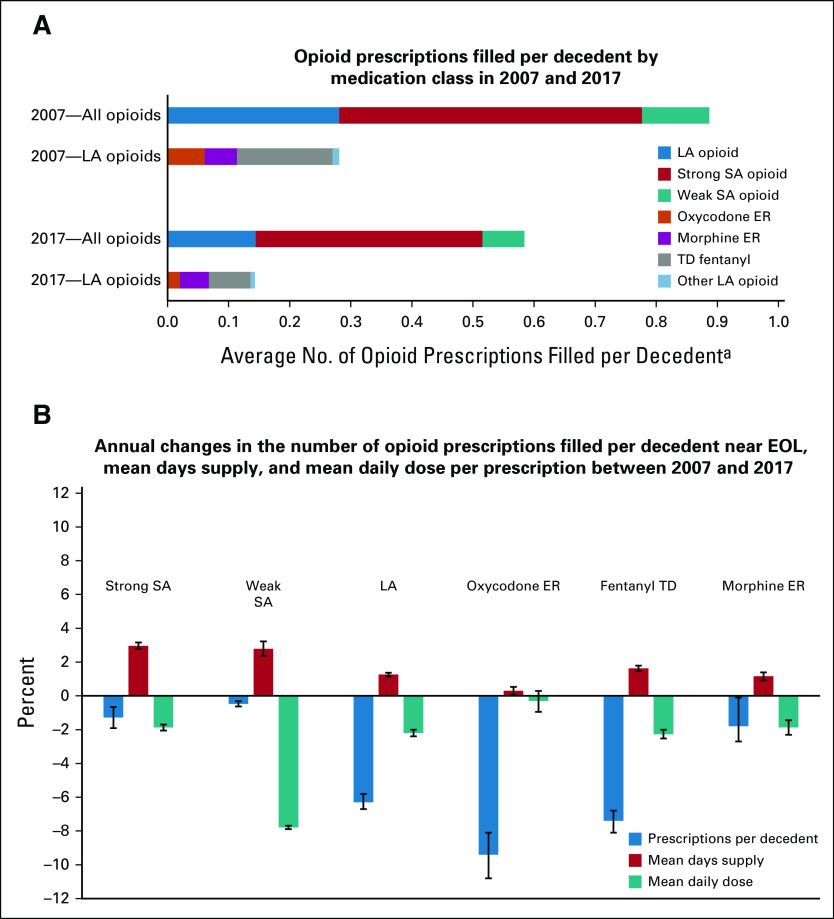
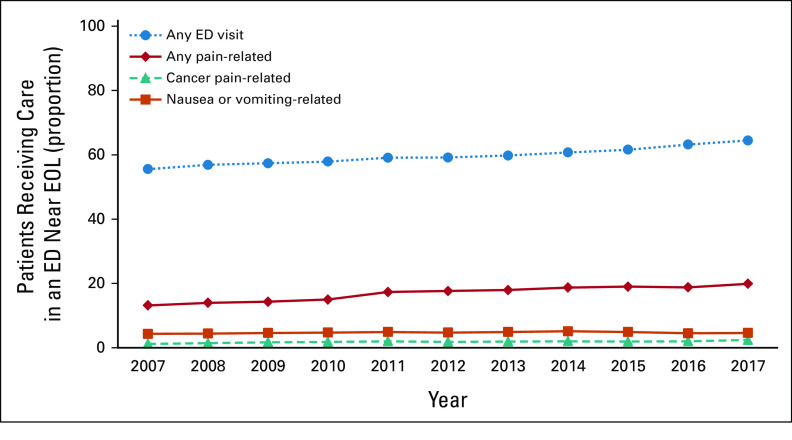
Results: Between 2007 and 2017, the proportion of decedents with poor prognosis cancers receiving ≥ 1 opioid prescription near EOL declined 15.5% (relative percent difference [RPD]), from 42.0% (95% CI, 41.4 to 42.7) to 35.5% (95% CI, 34.9 to 36.0) and the proportion receiving ≥ 1 long-acting opioid prescription declined 36.5% (RPD), from 18.1% (95% CI, 17.6 to 18.6) to 11.5% (95% CI, 11.1 to 11.9). Among decedents receiving opioids near EOL, the mean daily dose fell 24.5%, from 85.6 MMED (95% CI, 82.9 to 88.3) to 64.6 (95% CI, 62.7 to 66.6) MMED. Overall, the total amount of opioids prescribed per decedent near EOL (averaged across those who did and did not receive an opioid) fell 38.0%, from 1,075 morphine milligram equivalents per decedent (95% CI, 1,042 to 1,109) to 666 morphine milligram equivalents per decedent (95% CI, 646 to 686). Simultaneously, the proportion of patients with pain-related ED visits increased 50.8% (RPD), from 13.2% (95% CI, 12.7 to 13.6) to 19.9% (95% CI, 19.4 to 20.4). Sensitivity analyses demonstrated similar declines in opioid utilization in the 60 and 90 days before death or hospice, and suggested that trends in opioid access were not confounded by secular trends in hospice utilization.
Conclusion: Opioid use among patients dying of cancer has declined substantially from 2007 to 2017. Rising pain-related ED visits suggests that EOL cancer pain management may be worsening.
Conflict of interest statement
Figures
Comment in
-
Opioid Prescribing to Patients With Advanced Cancer: Unanswered Questions.J Clin Oncol. 2022 Jan 20;40(3):311-312. doi: 10.1200/JCO.21.02086. Epub 2021 Dec 8. J Clin Oncol. 2022. PMID: 34878802 No abstract available.
-
Reply to W. E. Rosa et al and T. N. Townsend et al.J Clin Oncol. 2022 Jan 20;40(3):312-314. doi: 10.1200/JCO.21.02383. Epub 2021 Dec 8. J Clin Oncol. 2022. PMID: 34878818 No abstract available.
-
The US Cancer Pain Crisis and the Global Pain Divide: Can Two Wrongs Make It Right?J Clin Oncol. 2022 Jan 20;40(3):310-311. doi: 10.1200/JCO.21.02049. Epub 2021 Dec 8. J Clin Oncol. 2022. PMID: 34878827 Free PMC article. No abstract available.
References
-
- Dart RC, Surratt HL, Cicero TJ, et al. :Trends in opioid analgesic abuse and mortality in the United States. N Engl J Med 372:241-248, 2015 - PubMed
-
- Bohnert AS, Valenstein M, Bair MJ, et al. :Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA 305:1315-1321, 2011 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
