

Safety, Efficacy, and Pharmacodynamics of Tremelimumab Plus Durvalumab for Patients With Unresectable Hepatocellular Carcinoma: Randomized Expansion of a Phase I/II Study
- PMID: 34292792
- PMCID: PMC8445563
- DOI: 10.1200/JCO.20.03555
Safety, Efficacy, and Pharmacodynamics of Tremelimumab Plus Durvalumab for Patients With Unresectable Hepatocellular Carcinoma: Randomized Expansion of a Phase I/II Study
Abstract
Purpose: This phase I/II study evaluated tremelimumab (anticytotoxic T-lymphocyte-associated antigen-4 monoclonal antibody) and durvalumab (antiprogrammed death ligand-1 monoclonal antibody) as monotherapies and in combination for patients with unresectable hepatocellular carcinoma (HCC), including a novel regimen featuring a single, priming dose of tremelimumab (ClinicalTrials.gov identifier: NCT02519348).
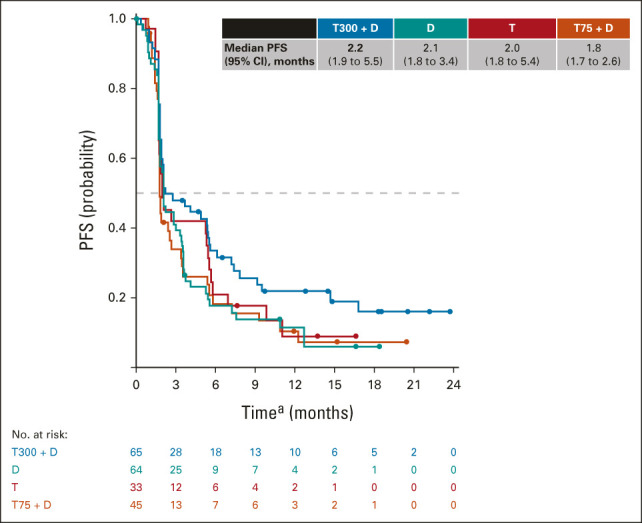
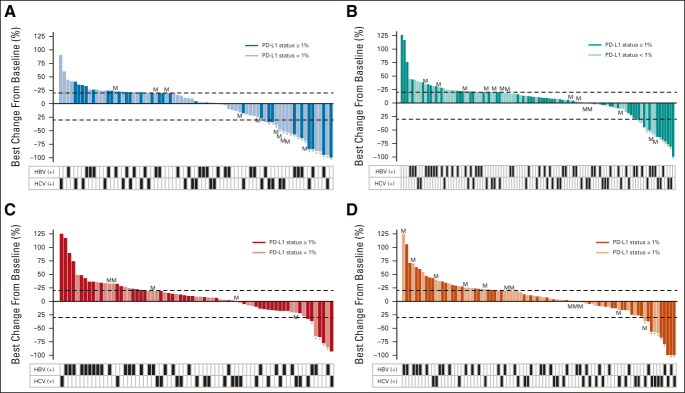
Patients and methods: Patients with HCC who had progressed on, were intolerant to, or refused sorafenib were randomly assigned to receive T300 + D (tremelimumab 300 mg plus durvalumab 1,500 mg [one dose each during the first cycle] followed by durvalumab 1,500 mg once every 4 weeks), durvalumab monotherapy (1,500 mg once every 4 weeks), tremelimumab monotherapy (750 mg once every 4 weeks [seven doses] and then once every 12 weeks), or T75 + D (tremelimumab 75 mg once every 4 weeks plus durvalumab 1,500 mg once every 4 weeks [four doses] followed by durvalumab 1,500 mg once every 4 weeks). Safety was the primary end point. Secondary end points included objective response rate (ORR) by Response Evaluation Criteria in Solid Tumors v1.1 and overall survival; exploratory end points included circulating lymphocyte profiles.
Results: A total of 332 patients were enrolled (T300 + D, n = 75; durvalumab, n = 104; tremelimumab, n = 69; and T75 + D, n = 84). Tolerability was acceptable across arms, with grade ≥ 3 treatment-related adverse events occurring in 37.8%, 20.8%, 43.5%, and 24.4%, respectively. Confirmed ORRs (95% CI) were 24.0% (14.9 to 35.3), 10.6% (5.4 to 18.1), 7.2% (2.4 to 16.1), and 9.5% (4.2 to 17.9), respectively. An early expansion of CD8+ lymphocytes was associated with response across arms, with highest proliferating CD8+ lymphocyte levels occurring in the T300 + D arm. The median (95% CI) overall survival was 18.7 (10.8 to 27.3), 13.6 (8.7 to 17.6), 15.1 (11.3 to 20.5), and 11.3 (8.4 to 15.0) months in the T300 + D, durvalumab, tremelimumab, and T75 + D arms, respectively.
Conclusion: All regimens were found to be tolerable and clinically active; however, the T300 + D regimen demonstrated the most encouraging benefit-risk profile. The unique pharmacodynamic activity and association with ORR of the T300 + D regimen further support its continued evaluation in HCC.
Conflict of interest statement
Figures









References
-
- Llovet JM Ricci S Mazzaferro V, et al. : Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 359:378-390, 2008 - PubMed
-
- Cheng AL Kang YK Chen Z, et al. : Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol 10:25-34, 2009 - PubMed
-
- Kudo M Finn RS Qin S, et al. : Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 391:1163-1173, 2018 - PubMed
-
- Finn RS Qin S Ikeda M, et al. : Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med 382:1894-1905, 2020 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
