

doi: 10.1161/CIRCRESAHA.121.319117.
Epub 2021 Jul 23.
SARS-CoV-2 Initiates Programmed Cell Death in Platelets
Affiliations
- PMID: 34293929
- PMCID: PMC8409903
- DOI: 10.1161/CIRCRESAHA.121.319117
Item in Clipboard
SARS-CoV-2 Initiates Programmed Cell Death in Platelets
Circ Res.
.
Abstract
[Figure: see text].
Keywords: COVID-19; SARS-CoV-2; apoptosis; blood platelets; extracellular vesicles; necroptosis; thrombosis.
Figures
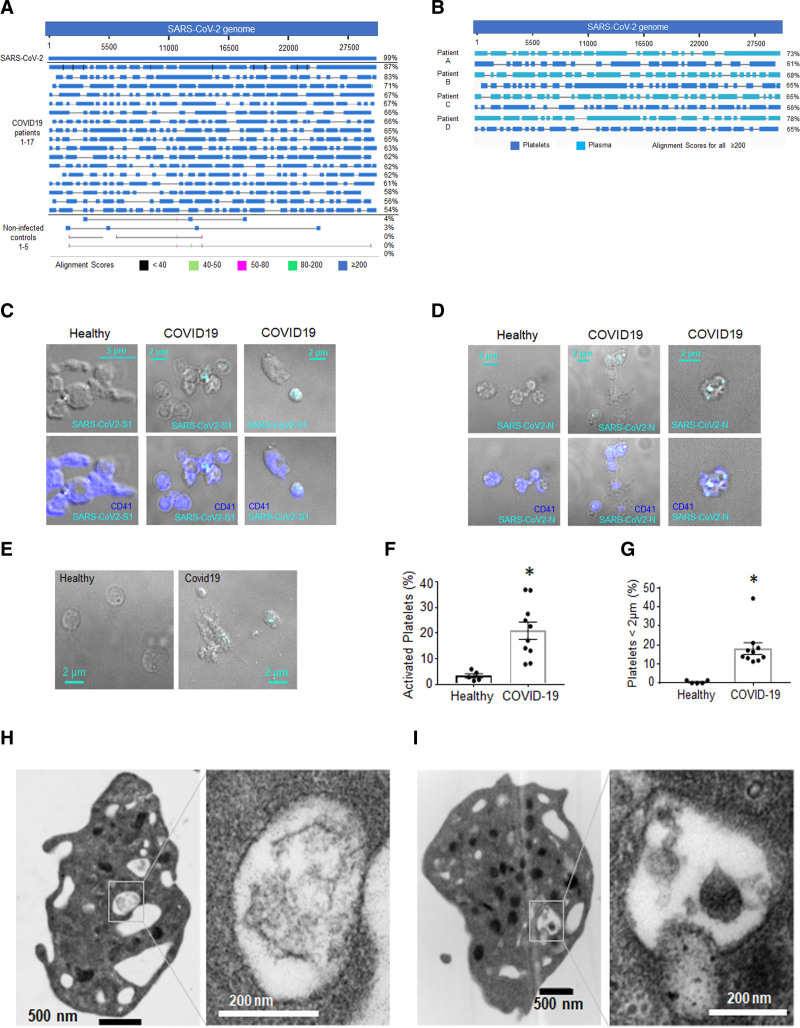
Detection of SARS-CoV-2 (severe acute respiratory syndrome, corona virus-2) in actively infected patients’ platelets.A and B, RNA from platelets from patients with coronavirus disease 2019 (COVID-19) and noninfected controls was sequenced using Artic V3 sequencing specifically enriching for the SARS-CoV-2 genome. RNA isolated from SARS-CoV-2 (USA-WA1/2020 Strain, BEI) was used as a positive control. Sequencing results were analyzed using Nucleotide Blast National Center for Biotechnology Information server against SARS-CoV-2 NC_045512_Wuhan-Hu-1 genome. A, Alignment of viral RNA (vRNA) in platelets. B, Alignment of vRNA in platelets (included in A) and plasma from the same patients. Whole blood from patients with COVID-19 was fixed and stained with antibodies against (C) SARS-CoV-2 Spike 1 protein and (D) SARS-CoV-2 Nucleocapsid protein with detection by immunofluorescence using spinning disk confocal microscopy and ×100 lens. E, Differential interference contrast (DIC) of healthy and COVID-19 platelets. Quantitation of (F) platelets that show severe activation and (G) platelets that are between 1 and 2 µm using confocal DIC images taken with ×100 (Covid-19: 2 females [F] and 3 males [M]). The healthy donors used here were n=5, 2M (56 y White participant; 44 y Asian); 3F (60 y White participant; 45 y White participant; 44 y White participant). Significance was assessed using a nonparametric test (Mann-Whitney), P=0.0079 for both graphs; data are presented as mean±SEM. H and I, Transmission electron microscopy of washed platelets from 2 different donors (representative of 6) showing structures that could be digested virus.
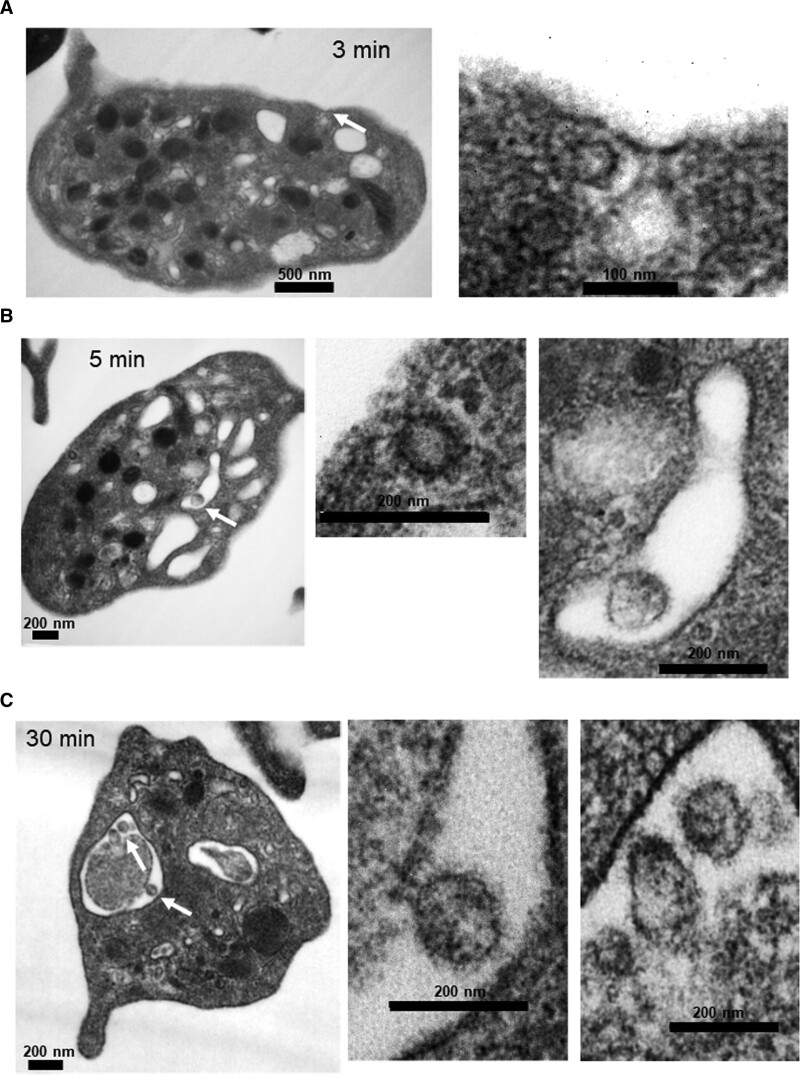
Platelets internalize infectious SARS-CoV-2 (severe acute respiratory syndrome, corona virus-2) in vitro. Infectious SARS-CoV-2 appears to be internalized by platelets via three distinct routes. Washed platelets from healthy human donors were incubated with SARS-CoV-2 virions (10:1) over time. Transmission electron microscopy shows that the virus can locate in (A) endosomes (only part of the virus), (B) in phagosome-like structures by itself (last image). Please note that the image in the middle is the size of a clathrin-coated vesicle and it is not a viral particle, and (C) in phagosome-like structures attached to platelet-derived microparticles.
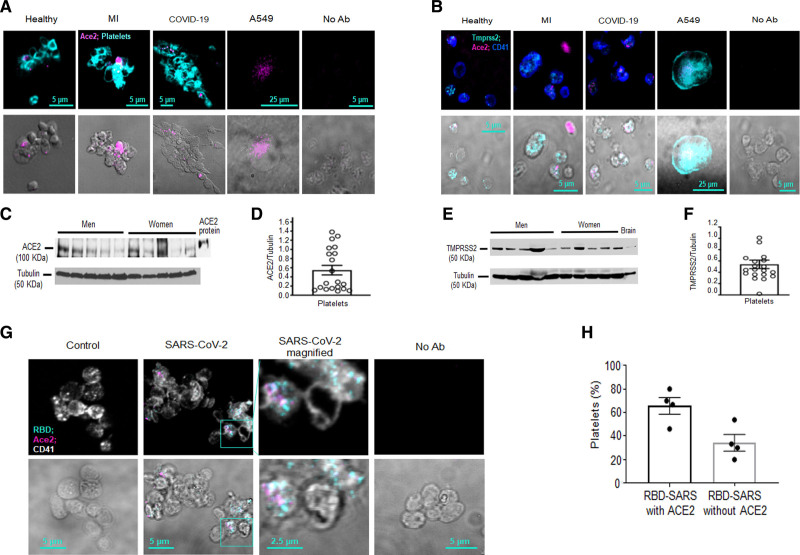
The binding domain of SARS-CoV-2 (severe acute respiratory syndrome, corona virus-2) does not always associate with ACE (angiotensin-converting enzyme) 2 on platelets.A and B, Platelets from whole blood were stained with ACE2 and CD41 postfixation of whole blood. Human alveolar epithelial cells (A549), transduced to stably overexpress ACE2 and TMPRSS2 (transmembrane serine protease 2), were used as a positive control. No antibody (Ab) control (No Ab) was used to account for autofluorescence of paraformaldehyde-fixed cells. A, Representative images of ACE2 expression in platelets from different donors. Healthy (n=4, 2 females [F] and 2 males [M]), myocardial infarction (MI; n=3, 2M, 1F), and coronavirus disease 2019 (COVID-19; n=6, 4M, 2F) donors were screened. B, ACE2 and TMPRSS2 colocalization in platelets from healthy, MI, and COVID-19 donors (representative images of n=4 healthy, n=3 with MI and n=4 with COVID-19). C–F, ACE2 and TMPRSS2 expression assessed by Western blot analysis of washed platelets from healthy human donors (blots are representative of n=20 healthy donors, 10M and 10F, age 40.1±2.8 y, all White participants); data are presented as mean±SEM. C, Representative Western blots of ACE2 and (D) densitometry of expression. E, TMPRSS2 Western blot and (F) Densitometry of expression. G, SARS-CoV-2 binds ACE2 on the platelet surface after viral incubation. Washed platelets from a healthy human donor were incubated for 5 min with SARS-CoV-2. Platelets were fixed and stained with Abs against ACE2 and the ACE2–receptor-binding domain (RBD) of the SARS-CoV-2 spike protein. H, Quantitation of platelets that have both SARS-CoV-2 and ACE2 vs. platelets that have only SARS-CoV-2 (n=4; 2M and 2F). The healthy donors used here were n=4, 2M (56 y White participant; 44 y Asian participant); 2F (59 y White participant; 46 y White participant). Significance was assessed using a nonparametric t test (Mann-Whitney), P values for all with * is 0.0289; data are presented as mean±SEM. Images and calculations are representative of n=4 different donors (2M and 2F).
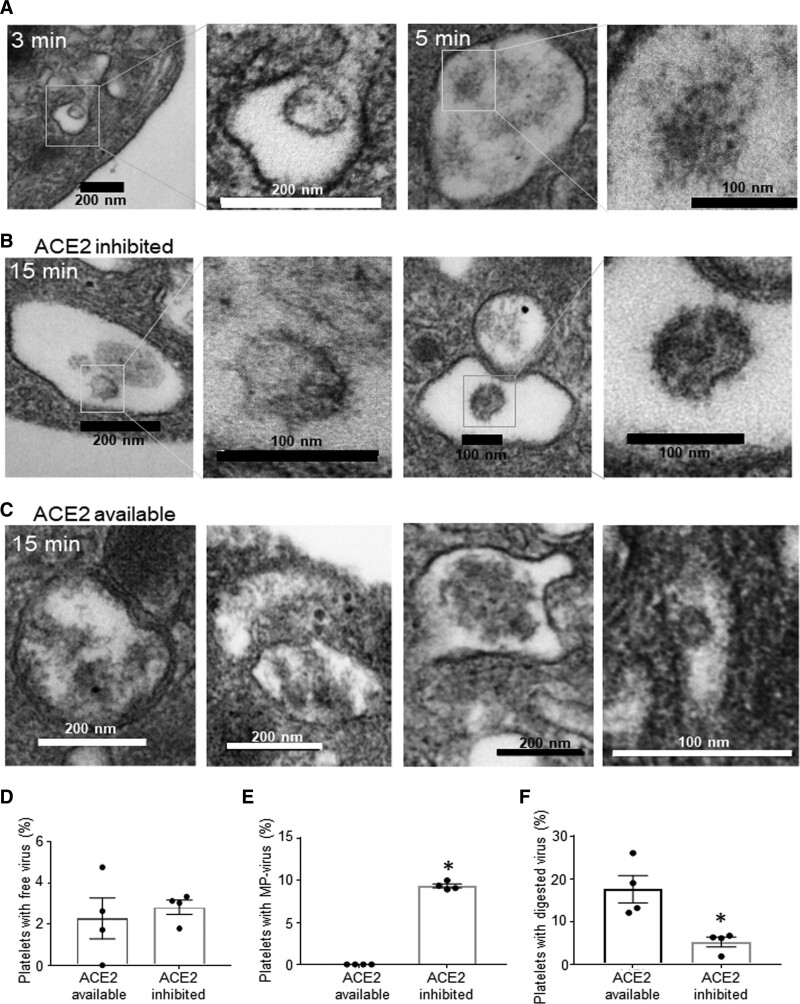
Platelets internalize SARS-CoV-2 (severe acute respiratory syndrome, corona virus-2) in ACE (angiotensin-converting enzyme) 2–dependent and ACE2-independent ways. Washed platelets from healthy human donors were incubated with SARS-CoV-2, and some were pretreated with DX600 (200 nmol/L) for 10 min. A, Platelets at 3–5 min in the absence of ACE2-inhibitor; platelets in (B) presence of and (C) absence of ACE2 inhibitor (DX600, 200 nmol/L) for 15 min at 37 °C and constant rotation at 1000 rpm (revolutions per minute). Samples were fixed with Karnovsky’s fixative and resolved by transmission electron microscopy. Quantitation of platelets from (B) and (C) showing (D) free virus, (E) virus attached to microparticles (MP), and (F) digested virus. Significance was assessed using a nonparametric t test (Mann-Whitney), P values for all with * is 0.0289; data are presented as mean±SEM. Images and calculations are representative of n=4 different donors (2 males [M] and 2 females [F]). The healthy donors used here were n=4, 2M (56 y White participant; 44 y Asian participant); 2F (59 y White participant; 46 y White participant).
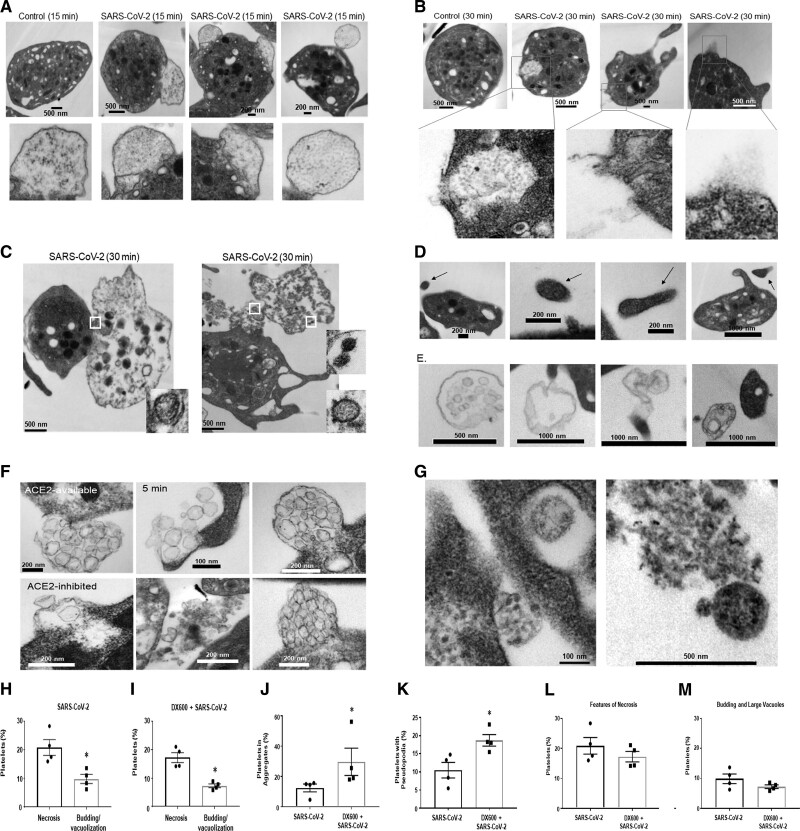
SARS-CoV-2 (severe acute respiratory syndrome, corona virus-2) mediates distinct morphological changes in platelets and various forms of extracellular vesicle release. Washed platelets from healthy human donors were incubated with SARS-CoV-2 virions (10:1) for various time points. Transmission electron microscopy shows that SARS-CoV-2 leads to (A) budding (B) content release from broken membrane or channels; presence of degranulates, and (C) necrotic platelets; (D) platelet microparticles; (E) migrasomes; (F) exosome release; (G) intracellular platelet content release of nongranule origin. H–M, Quantification of Transmission electron microscopy images from n=4 healthy donors at 15 min in the presence and absence of ACE (angiotensin-converting enzyme) 2 inhibitor; necrotic features were defined as empty platelets with broken membranes. The healthy donors used here were n=4, 2 males (M; 56 y White participant; 44 y Asian participant); 2 females (F; 60 y White participant; 46 y White participant). Significance was assessed using a nonparametric t test (Mann-Whitney), P values for all with * is 0.0289; data are presented as mean±SEM. SARS-CoV-2 indicates severe acute respiratory syndrome, corona virus 2.
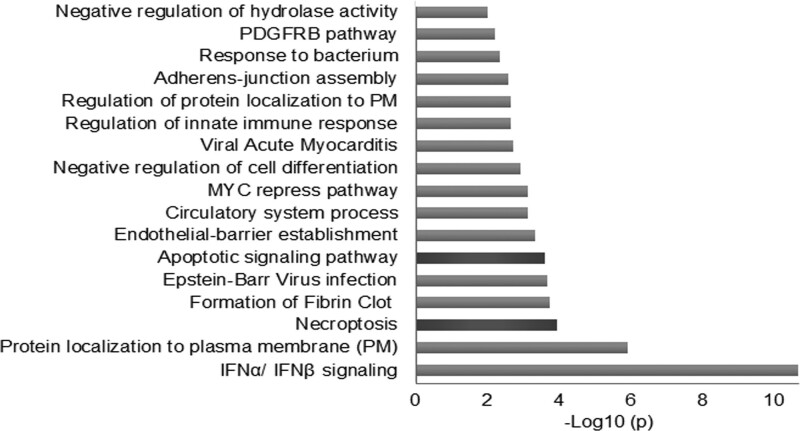
Pathway enrichment analysis of coronavirus disease 2019 (COVID-19) platelet transcriptome suggests programmed cell death. Platelets from patients with COVID-19 (n=10) and patients with myocardial infarction (ST-segment–elevation myocardial infarction [n=10], non–ST-segment–elevation myocardial infarction [n=10]) without COVID-19 were isolated and sequenced. Pathway enrichment analyses, with the respective P values were generated in https://metascape.org/ using the fold changes from the RNAseq (RNA sequencing) data of the highest, statistically significant, 40 upregulated, and 40 downregulated genes. Fold changes of the sequencing results are included in Table VII in the Data Supplement . IFN indicates interferon. MYC indicates myelocytomatosis; PDGFRB, platelet-derived growth factor receptor beta; and PM, plasma membrane.
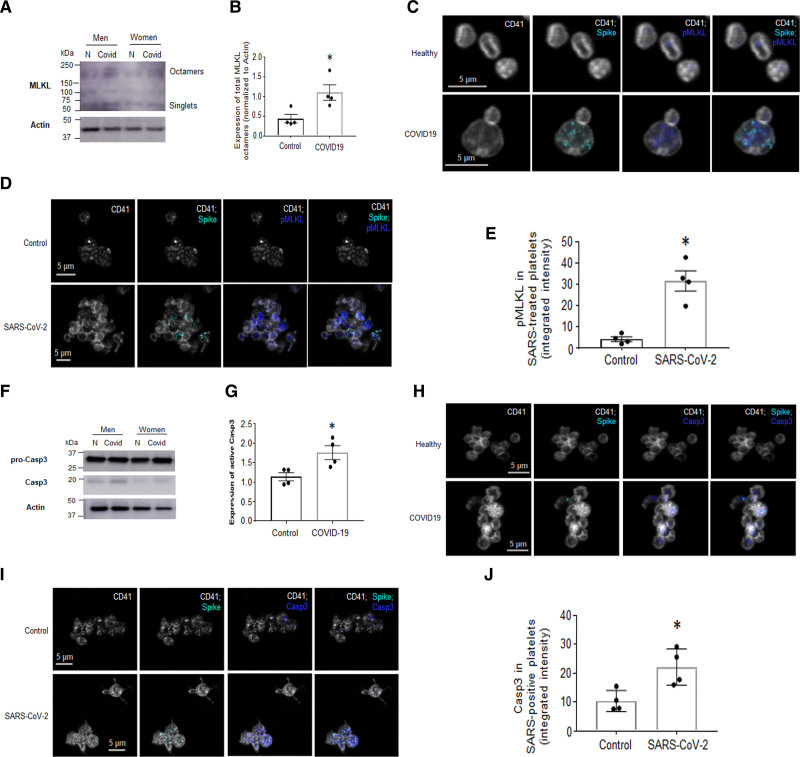
Platelets from patients with coronavirus disease 2019 (COVID-19), and platelets from healthy donors treated with SARS-CoV-2 (severe acute respiratory syndrome, corona virus-2), have upregulated markers of programmed cell death. Washed platelets from patients with COVID-19 were subjected to Western blot (WB) analysis. Markers for necroptosis (A) MLKL (mixed lineage kinase domain-like pseudokinase)-octamer formation by WB (representative images of n=4, 3 males [M], 1 female [F]; the images shown here are from sex- and age-matched groups that include a male and a female pair). B, Quantification of A. C and D, Colocalization of SARS-CoV-2 with p-MLKL (phosphorylated MLKL) by immunofluorescence (IF). C, In COVID-19 blood and in D. Platelets postincubation with SARS-CoV-2 for 30 min. E, Quantitation of D using integrated intensity over platelet number (ImageJ). Marker for apoptosis. F, Active Casp3 (caspase 3) expression (representative images of n=4, 3M, 1F; the images shown here are from sex- and age-matched groups that include a male and a female pair) and its (G) quantitation and H and I. Colocalization of SARS-CoV-2 and Casp 3 in platelets in H. Whole blood from patients with COVID-19 and (I) platelets incubated with SARS-CoV-2 for 30 min by IF; (J) quantitation of I as in E. IF was performed on whole blood that was immediately RBC-lysed and fixed with 4% paraformaldehyde and then stained with the indicated markers (platelet marker used is CD41). IF images are representative of n=4 different patients with COVID-19 on n=4 different healthy donors. Significance was assessed using a nonparametric t test (Mann-Whitney), *P values for B and G are 0.0289; *P values for E and J are 0.0286; data are presented as mean±SEM.
Comment in
-
Are Platelets SARS-CoV-2's "Dead End"?Circ Res. 2021 Sep 3;129(6):647-649. doi: 10.1161/CIRCRESAHA.121.319913. Epub 2021 Sep 2. Circ Res. 2021. PMID: 34473529 No abstract available.
References
-
- Petrilli CM, Jones SA, Yang J, Rajagopalan H, O’Donnell L, Chernyak Y, Tobin KA, Cerfolio RJ, Francois F, Horwitz LI. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ. 2020;369:m1966. doi: 10.1136/bmj.m1966 - PMC - PubMed
-
- McGurnaghan SJ, Weir A, Bishop J, Kennedy S, Blackbourn LAK, McAllister DA, Hutchinson S, Caparrotta TM, Mellor J, Jeyam A, et al. ; Public Health Scotland COVID-19 Health Protection Study Group; Scottish Diabetes Research Network Epidemiology Group. Risks of and risk factors for COVID-19 disease in people with diabetes: a cohort study of the total population of Scotland. Lancet Diabetes Endocrinol. 2021;9:82–93. doi: 10.1016/S2213-8587(20)30405-8 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
