

Association of blood pressure and renal outcome in patients with chronic kidney disease; a post hoc analysis of FROM-J study
- PMID: 34294784
- PMCID: PMC8298520
- DOI: 10.1038/s41598-021-94467-z
Association of blood pressure and renal outcome in patients with chronic kidney disease; a post hoc analysis of FROM-J study
Abstract
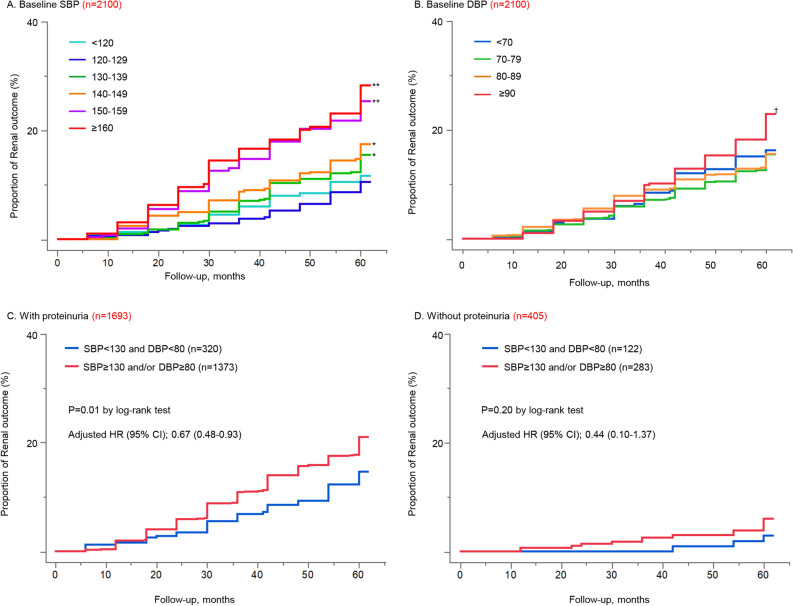
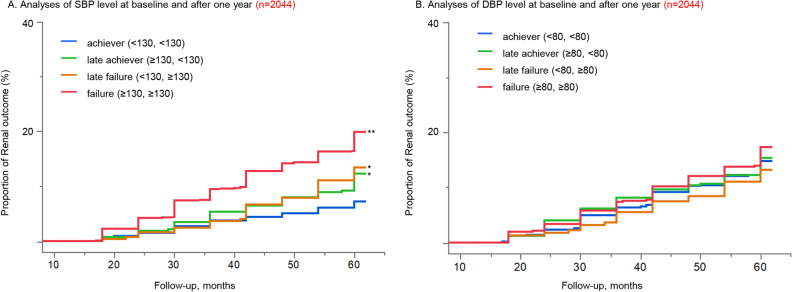
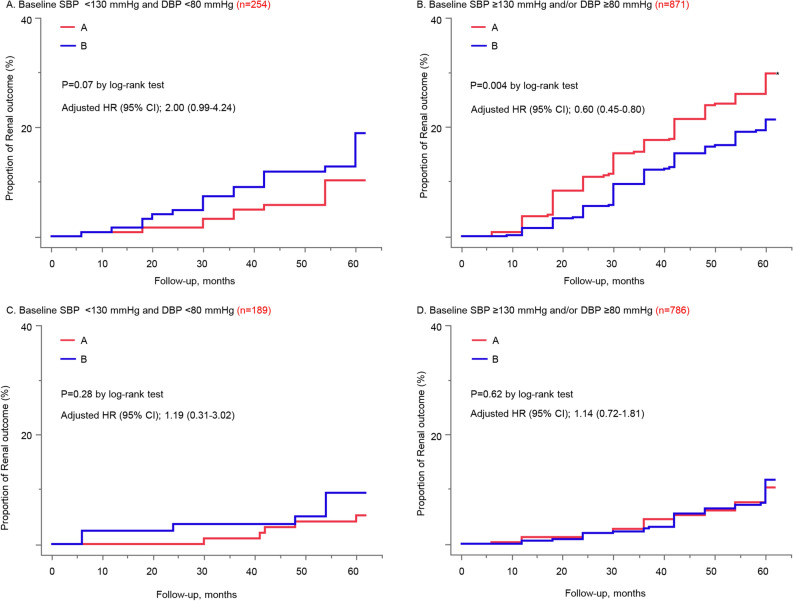
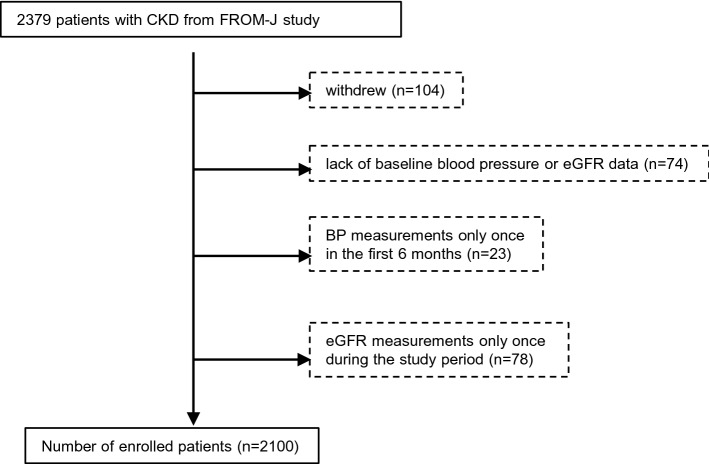
It is well-known that hypertension exacerbates chronic kidney disease (CKD) progression, however, the optimal target blood pressure (BP) level in patients with CKD remains unclear. This study aimed to assess the optimal BP level for preventing CKD progression. The risk of renal outcome among different BP categories at baseline as well as 1 year after, were evaluated using individual CKD patient data aged between 40 and 74 years from FROM-J [Frontier of Renal Outcome Modifications in Japan] study. The renal outcome was defined as ≥ 40% reduction in estimated glomerular filtration rate to < 60 mL/min/1.73 m2, or a diagnosis of end stage renal disease. Regarding baseline BP, the group of systolic BP (SBP) 120-129 mmHg had the lowest risk of the renal outcome, which increased more than 60% in SBP ≥ 130 mmHg group. A significant increase in the renal outcome was found only in the group of diastolic BP ≥ 90 mmHg. The group of BP < 130/80 mmHg had a benefit for lowering the risk regardless of the presence of proteinuria, and it significantly reduced the risk in patients with proteinuria. Achieving SBP level < 130 mmHg after one year resulted in a 42% risk reduction in patients with SBP level ≥ 130 mmHg at baseline. Targeting SBP level < 130 mmHg would be associated with the preferable renal outcome.Clinical Trial Registration-URL: https://www.umin.ac.jp/ctr/ . Unique identifier: UMIN000001159 (16/05/2008).
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
