

Management of biliary diseases after the failure of initial needle knife precut sphincterotomy for biliary cannulation
- PMID: 34294788
- PMCID: PMC8298459
- DOI: 10.1038/s41598-021-94361-8
Management of biliary diseases after the failure of initial needle knife precut sphincterotomy for biliary cannulation
Abstract
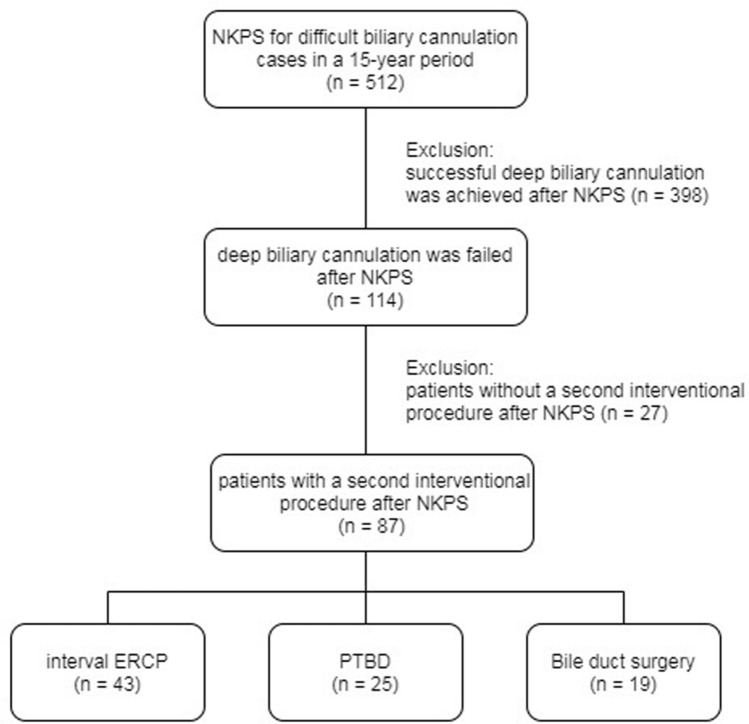
Endoscopic retrograde cholangiopancreatography is not always successful even with needle knife precut sphincterotomy (NKPS). How to manage these patients with initial NKPS failure has not been well studied. We report the outcomes of patients who received endoscopic and non-endoscopic rescue treatment after the initial NKPS failure. During the 15 years from 2004 to 2018, 87 patients with initial NKPS failure received interval endoscopic treatment (IET group, n = 43), percutaneous transhepatic biliary drainage (PTBD group, n = 25), or bile duct surgery (BDS group, n = 19) were retrospectively studied. Compared with the PTBD group, the prevalence of choledocholithiasis was higher (69.8% vs. 16.0%, p < 0.001), and malignant bile duct stricture were lower (20.9% vs. 76.0%, p < 0.001) in the IET group. Furthermore, the IET group had a significantly longer time interval between the first and second treatment procedures (4 days vs. 2 days, p = 0.001), a lower technique success rate (79.1% vs. 100%, p = 0.021), and a shorter length of hospital stay (7 days vs. 18 days, p < 0.001). Compared to the BDS group, the only significant finding was that the patients in the IET group were older. Although not statistically significant, the complication rate was lowest in the IET group (7.0%) while highest in the BDS group (15.8%). Complications in the IET group were also mild, as compared with the other two groups. In conclusion, IET should be considered after initial failed NKPS for deep biliary cannulation before contemplating more invasive treatment such as BDS. PTBD may be the alternative therapy for patients with malignant biliary obstruction.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Comparison of sequential pancreatic duct guidewire placement technique and needle knife precut sphincterotomy for difficult biliary cannulation.J Dig Dis. 2015 Dec;16(12):741-6. doi: 10.1111/1751-2980.12300. J Dig Dis. 2015. PMID: 26562073
-
Transpancreatic precut sphincterotomy for cannulation of inaccessible common bile duct: a safe and successful technique.Pancreas. 2008 Mar;36(2):187-91. doi: 10.1097/MPA.0b013e31815ac54c. Pancreas. 2008. PMID: 18376311
-
Difficult biliary cannulation: use of physician-controlled wire-guided cannulation over a pancreatic duct stent to reduce the rate of precut sphincterotomy (with video).Gastrointest Endosc. 2010 Feb;71(2):275-9. doi: 10.1016/j.gie.2009.08.028. Epub 2009 Nov 18. Gastrointest Endosc. 2010. PMID: 19922927
-
Management of difficult or failed biliary access in initial ERCP: A review of current literature.Clin Res Hepatol Gastroenterol. 2019 Aug;43(4):365-372. doi: 10.1016/j.clinre.2018.09.004. Epub 2018 Oct 9. Clin Res Hepatol Gastroenterol. 2019. PMID: 30314736 Review.
-
[Needle-knife sphincterotomy for biliary access: a prospective study].Gastroenterol Hepatol. 2005 Aug-Sep;28(7):369-74. doi: 10.1157/13077756. Gastroenterol Hepatol. 2005. PMID: 16137469 Review. Spanish.
Cited by
-
Endoscopic salvage therapy after failed biliary cannulation using advanced techniques: A concise review.World J Gastroenterol. 2022 Aug 7;28(29):3803-3813. doi: 10.3748/wjg.v28.i29.3803. World J Gastroenterol. 2022. PMID: 36157537 Free PMC article. Review.
-
Analysis of the Effectiveness of Second Attempt Endoscopic Retrograde Cholangiopancreatography (ERCP) 24 Hours (Second Day) After Primary Failure.Cureus. 2024 Feb 1;16(2):e53405. doi: 10.7759/cureus.53405. eCollection 2024 Feb. Cureus. 2024. PMID: 38435233 Free PMC article.
-
Second endoscopic retrograde cholangiopancreatography after failure of initial biliary cannulation: A single institution retrospective experience.Exp Ther Med. 2022 Apr;23(4):297. doi: 10.3892/etm.2022.11226. Epub 2022 Feb 18. Exp Ther Med. 2022. PMID: 35340881 Free PMC article.
-
Predictive factors of needle-knife pre-cut papillotomy failure in patients with difficult biliary cannulation.Sci Rep. 2022 Mar 23;12(1):4942. doi: 10.1038/s41598-022-09117-9. Sci Rep. 2022. PMID: 35322178 Free PMC article.
References
-
- Sundaralingam P, Masson P, Bourke MJ. Early precut sphincterotomy does not increase risk during endoscopic retrograde cholangiopancreatography in patients with difficult biliary access: A meta-analysis of randomized controlled trials. Clin. Gastroenterol. Hepatol. 2015;13:1722–1729.e1722. doi: 10.1016/j.cgh.2015.06.035. - DOI - PubMed
-
- Ang TL, Kwek AB, Lim KB, Teo EK, Fock KM. An analysis of the efficacy and safety of a strategy of early precut for biliary access during difficult endoscopic retrograde cholangiopancreatography in a general hospital. J. Dig. Dis. 2010;11:306–312. doi: 10.1111/j.1751-2980.2010.00454.x. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
