

Lower synaptic density is associated with psychiatric and cognitive alterations in obesity
- PMID: 34294874
- PMCID: PMC8674236
- DOI: 10.1038/s41386-021-01111-5
Lower synaptic density is associated with psychiatric and cognitive alterations in obesity
Abstract
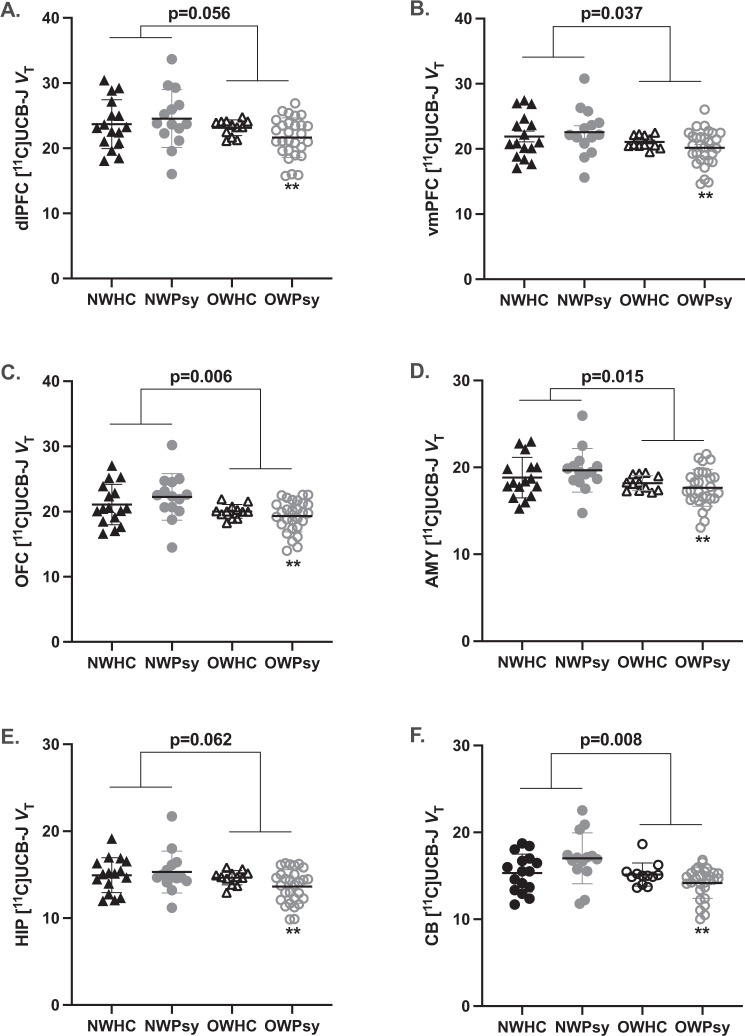
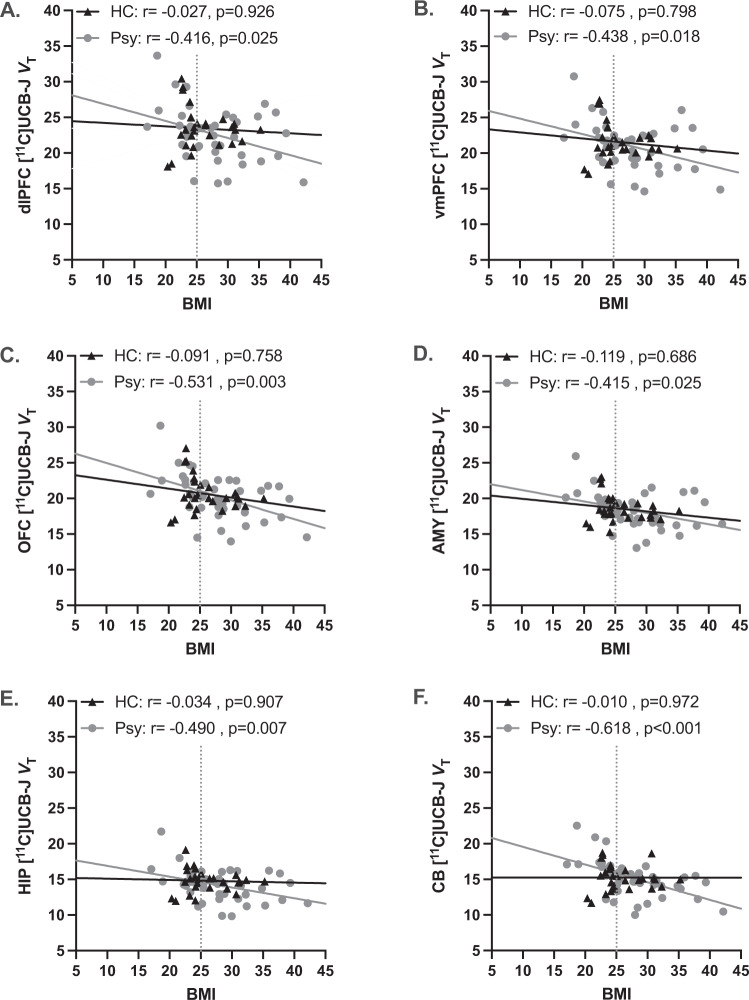
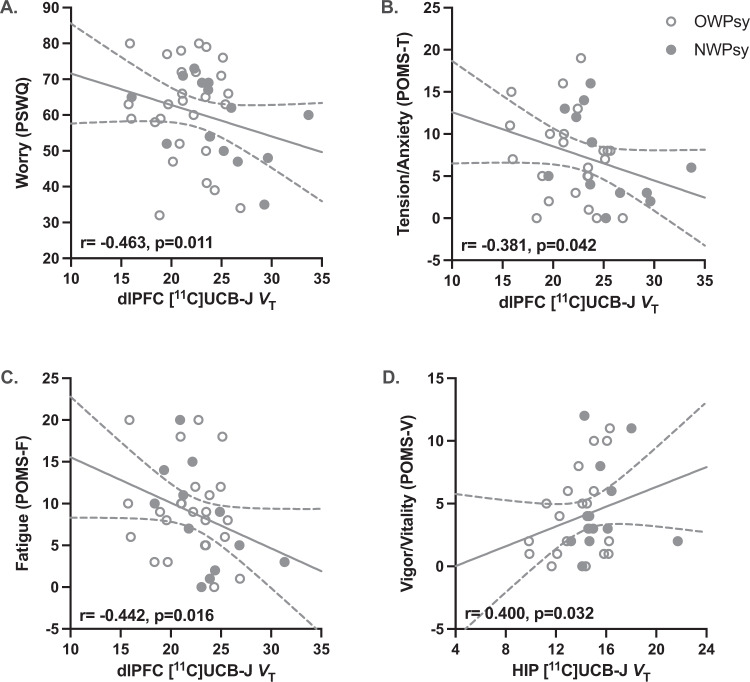
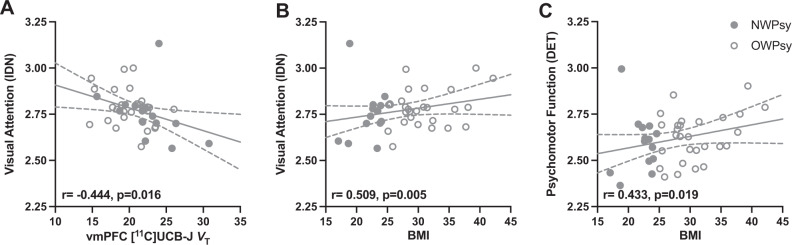
Obesity is a serious medical condition that often co-occurs with stress-related psychiatric disorders. It is recognized that the brain plays a key role in the (patho)physiology of obesity and that there is a bidirectional relationship between obesity and psychopathology, yet molecular mechanisms altered in obesity have not been fully elucidated. Thus, we investigated relationships between obesity and synaptic density in vivo using the radioligand [11C]UCB-J (which binds to synaptic glycoprotein SV2A) and positron emission tomography in individuals with obesity, and with or without stress-related psychiatric disorders. Regions of interest were the dorsolateral prefrontal cortex, orbitofrontal cortex, ventromedial, amygdala, hippocampus, and cerebellum. Forty individuals with a body mass index (BMI) ≥ 25 kg/m2 (overweight/obese), with (n = 28) or without (n = 12) psychiatric diagnosis, were compared to 30 age- and sex-matched normal weight individuals (BMI < 25), with (n = 14) or without (n = 16) psychiatric diagnosis. Overall, significantly lower synaptic density was observed in overweight/obese relative to normal weight participants (ηp2 = 0.193, F = 2.35, p = 0.042). Importantly, in participants with stress-related psychiatric diagnoses, we found BMI to be negatively correlated with synaptic density in all regions of interest (p ≤ 0.03), but no such relationship observed for mentally healthy controls (p ≥ 0.68). In the stress-related psychiatric groups, dorsolateral prefrontal cortex synaptic density was negatively associated with measures of worry (r = -0.46, p = 0.01), tension/anxiety (r = -0.38, p = 0.04), fatigue (r = -0.44, p = 0.02), and attentional difficulties (r = -0.44, p = 0.02). In summary, the findings of this novel in vivo experiment suggest compounding effects of obesity and stress-related psychopathology on the brain and the associated symptomatology that may impact functioning. This offers a novel biological mechanism for the relationship between overweight/obesity and stress-related psychiatric disorders that may guide future intervention development efforts.
© 2021. The Author(s), under exclusive licence to American College of Neuropsychopharmacology.
Figures
References
-
- World Health Organization. Obesity and overweight. 2020. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Accessed 15 Feb 2021.
-
- Centers for Disease Control and Prevention. Defining adult overweight and obesity. 2020. https://www.cdc.gov/obesity/adult/defining.html. Accessed 11 Nov 2020.
-
- Ward ZJ, Bleich SN, Cradock AL, Barrett JL, Giles CM, Flax C, et al. Projected U.S. State-level prevalence of adult obesity and severe obesity. N Engl J Med. 2019;381:2440–50. - PubMed
-
- Koliaki C, Liatis S, Kokkinos A. Obesity and cardiovascular disease: revisiting an old relationship. Metabolism. 2019;92:98–107. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
