

Autoimmune biliary diseases: primary biliary cholangitis and primary sclerosing cholangitis
- PMID: 34294935
- PMCID: PMC8299325
- DOI: 10.32074/1591-951X-245
Autoimmune biliary diseases: primary biliary cholangitis and primary sclerosing cholangitis
Abstract
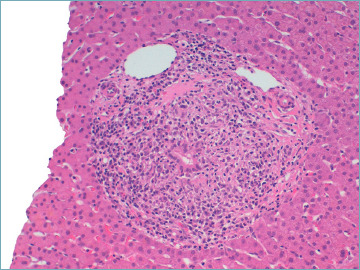
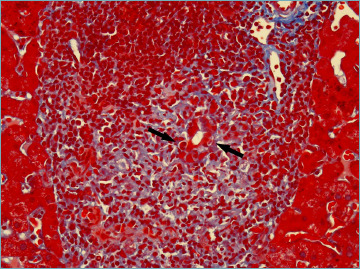
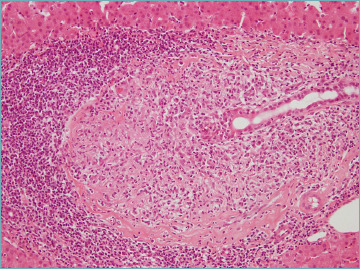
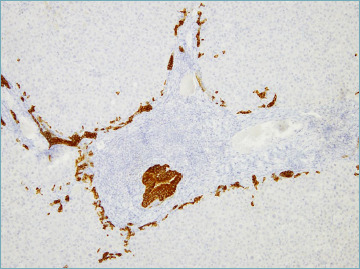
Autoimmune cholestatic liver diseases are rare hepato-biliary disorders characterized by a progressive, inflammatory destruction of bile ducts. Primary biliary cholangitis (PBC) and primary sclerosing cholangitis (PSC) are the main autoimmune cholestatic liver diseases. Both may evolve into secondary biliary cirrhosis and its complications. Therapeutic options are limited and liver transplantation remains the only definitive treatment for PBC and PSC.
Most PBC and PSC patients have a typical presentation, which does not require liver biopsy. However, in routine clinical practice, important variants or specific subgroups that benefit from liver biopsy for proper management may be observed. Herein, we provide a general overview of clinical and pathological characteristic of PBC and PSC, highlighting the most important features for routine diagnostic practice.
Keywords: PBC; PSC; autoimmune cholangitis; immune-mediated cholangitis; overlap variants.
Copyright © 2021 Società Italiana di Anatomia Patologica e Citopatologia Diagnostica, Divisione Italiana della International Academy of Pathology.
Conflict of interest statement
The Authors declare no conflict of interest.
Figures
References
-
- Lazaridis KN, LaRusso NF. The cholangiopathies. Mayo Clin Proc 2015;90:791-800. https://doi.org/10.1016/j.mayocp.2015.03.017 10.1016/j.mayocp.2015.03.017 - DOI - PMC - PubMed
-
- Lazaridis KN, Strazzabosco M, Larusso NF. The cholangiopathies: disorders of biliary epithelia. Gastroenterology 2004;127:1565-1577. https://doi.org/10.1053/j.gastro.2004.08.006 10.1053/j.gastro.2004.08.006 - DOI - PubMed
-
- Dalekos GN, Gatselis NK. Variant and specific forms of autoimmune cholestatic liver diseases. Arch Immunol Ther Exp (Warsz) 2019;67:197-211. https://doi.org/10.1007/s00005-019-00550-9 10.1007/s00005-019-00550-9 - DOI - PubMed
-
- Harada K, Sato Y, Itatsu K, et al. . Innate immune response to double-stranded RNA in biliary epithelial cells is associated with the pathogenesis of biliary atresia. Hepatology 2007;46:1146-1154. https://doi.org/10.1002/hep.21797 10.1002/hep.21797 - DOI - PubMed
-
- Nakanuma Y, Zen Y. Pathology and immunopathology of immunoglobulin G4-related sclerosing cholangitis: the latest addition to the sclerosing cholangitis family. Hepatol Res 2007;37:S478-486. https://doi.org/10.1111/j.1872-034X.2007.00243.x 10.1111/j.1872-034X.2007.00243.x - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
