

Nomograms for Predicting Overall Survival Among Patients with Craniopharyngiomas at Initial Diagnosis: A SEER Population-Based Analysis
- PMID: 34295180
- PMCID: PMC8290489
- DOI: 10.2147/IJGM.S320643
Nomograms for Predicting Overall Survival Among Patients with Craniopharyngiomas at Initial Diagnosis: A SEER Population-Based Analysis
Abstract
Background: Craniopharyngiomas (CPs) are relatively rare benign tumor located in the central nervous system (CNS). This study investigates the related risk factors of survival of craniopharyngiomas and develops a simple but detailed method predicting prognosis based on the Surveillance, Epidemiology, and End Results (SEER) database in order to improve the clinic management of CPs.
Methods: Between 2004 and 2017, 1213 patients diagnosed with craniopharyngiomas registered at the program and were included in the SEER-21 registry database. Overall survival (OS) curves were plotted with the Kaplan-Meier method and significance was determined by Log rank test. Single- and multiple-factor regression analyses were made using Cox proportional hazards model to identify independent predictors related to OS. Subsequently, we developed a nomogram with those factors to predict 3-, 5- and 10-year OS of craniopharyngiomas patients.
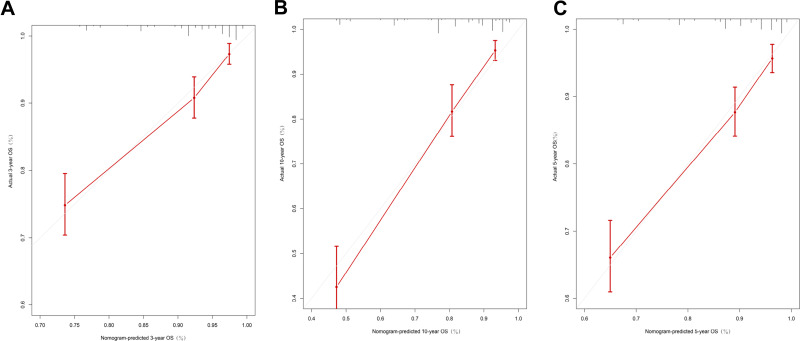
Results: We identified 1213 patients with craniopharyngioma. The OS rates at 3, 5, and 10 years after diagnosis were 89.1%, 86.2%, and 83%. Age, ethnicity, tumor size and radiation therapy were confirmed to be predictors correlating with OS at initial diagnosis. In multivariate analysis, we found that younger age (P<0.001), smaller tumor size (P<0.001), white ethnicity (P<0.001) and radiation therapy (P=0.004) were the factors that remained significantly associated with better survival. A nomogram was successfully constructed and validated by ROC, calibration plots and C-index of 0.773 (95% CI, 0.708-0.838).
Conclusion: The well-calibrated nomogram is the first clinical prediction model for predicting the prognosis for patients with craniopharyngiomas at initial diagnosis. Our study indicates that the surgical effect is not clear. Younger white patients with radiotherapy have a better prognosis, and the gross total resection (GTR) was not effective in prolonging the OS of a patient compared to no surgery and subtotal resection (STR).
Keywords: SEER; craniopharyngioma; nomogram; overall survival.
© 2021 Teng et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures




References
-
- Muller HL, Merchant TE, Warmuth-Metz M, Martinez-Barbera JP, Puget S. Craniopharyngioma. Nat Rev Dis Primers. 2019;5(1):75. - PubMed
-
- Pereira AM, Schmid EM, Schutte PJ, et al. High prevalence of long-term cardiovascular, neurological and psychosocial morbidity after treatment for craniopharyngioma. Clin Endocrinol. 2005;62(2):197–204. - PubMed
-
- Karavitaki N, Brufani C, Warner JT. Craniopharyngiomas in children and adults: systematic analysis of 121 cases with long-term follow-up. Clin Endocrinol. 2005;62(4):397–409. - PubMed
LinkOut - more resources
Full Text Sources
