

June: open-source individual-based epidemiology simulation
- PMID: 34295529
- PMCID: PMC8261230
- DOI: 10.1098/rsos.210506
June: open-source individual-based epidemiology simulation
Abstract
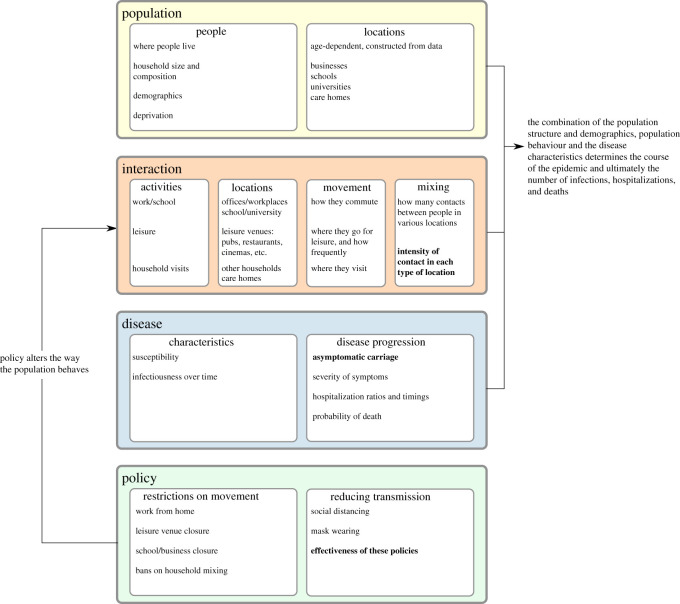
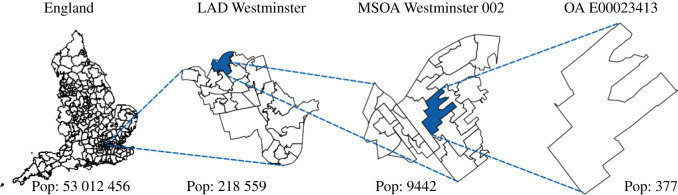
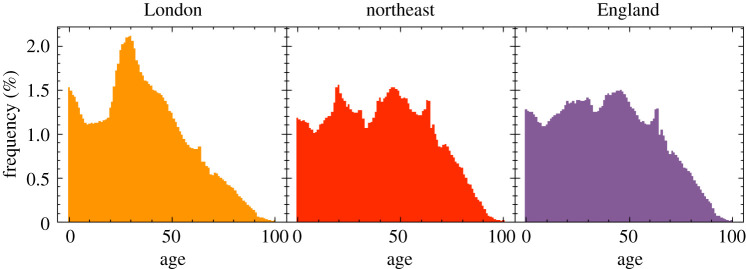
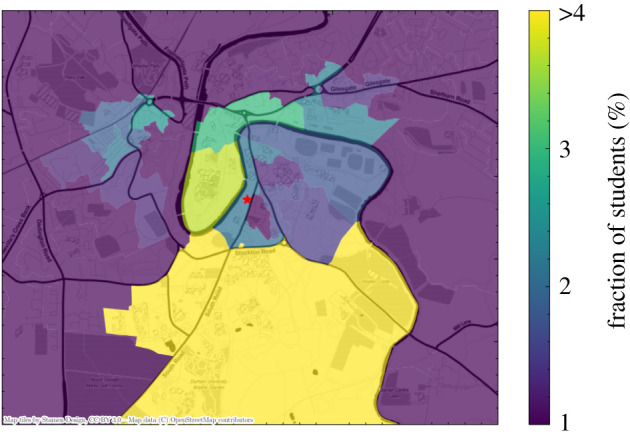
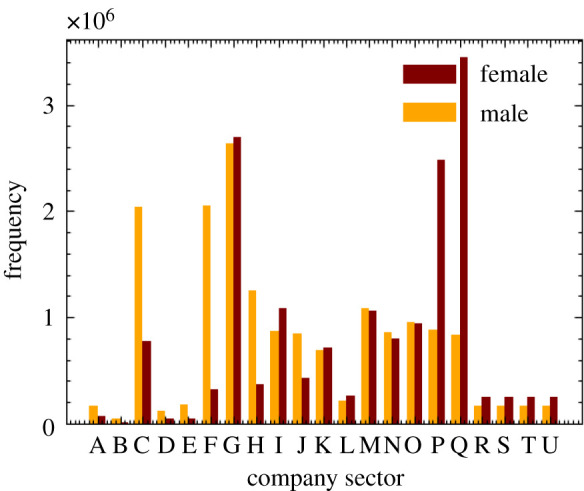
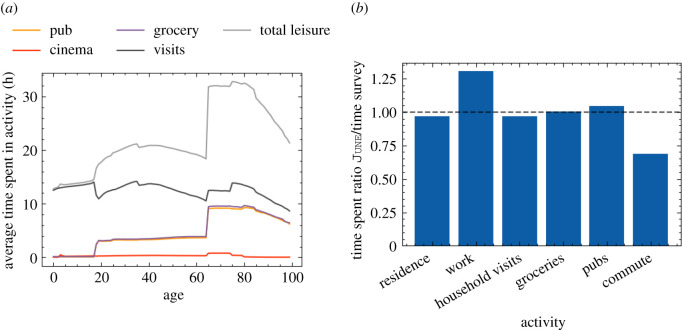
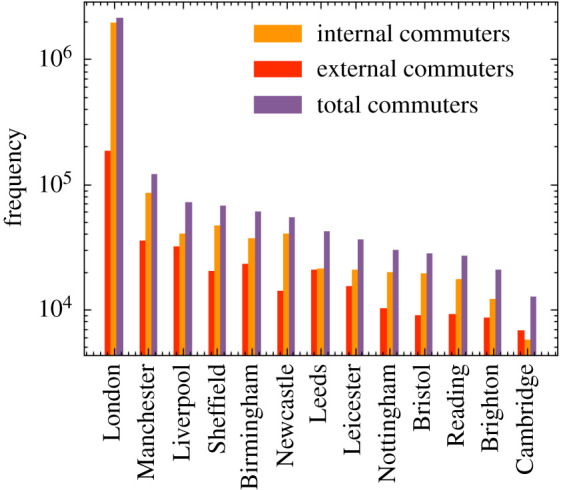
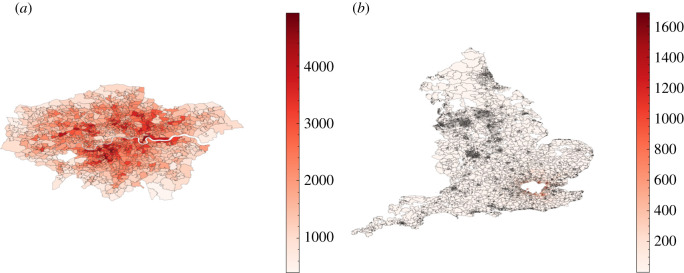
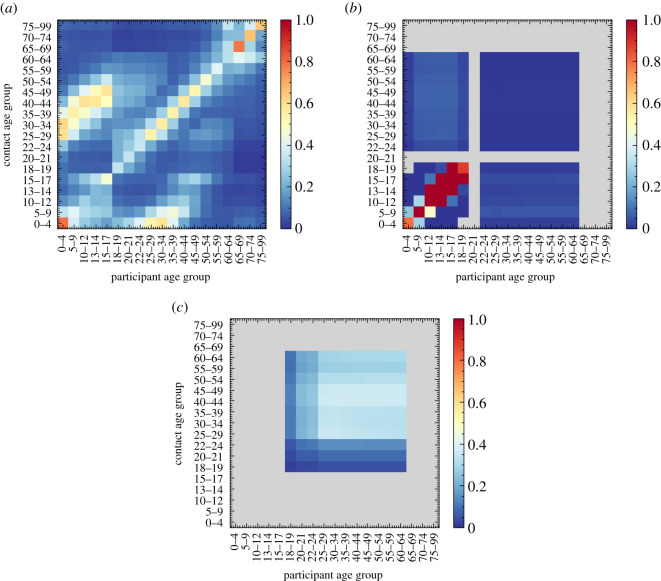
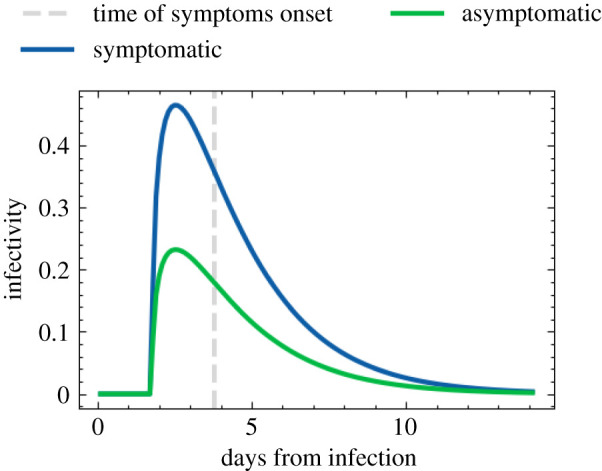
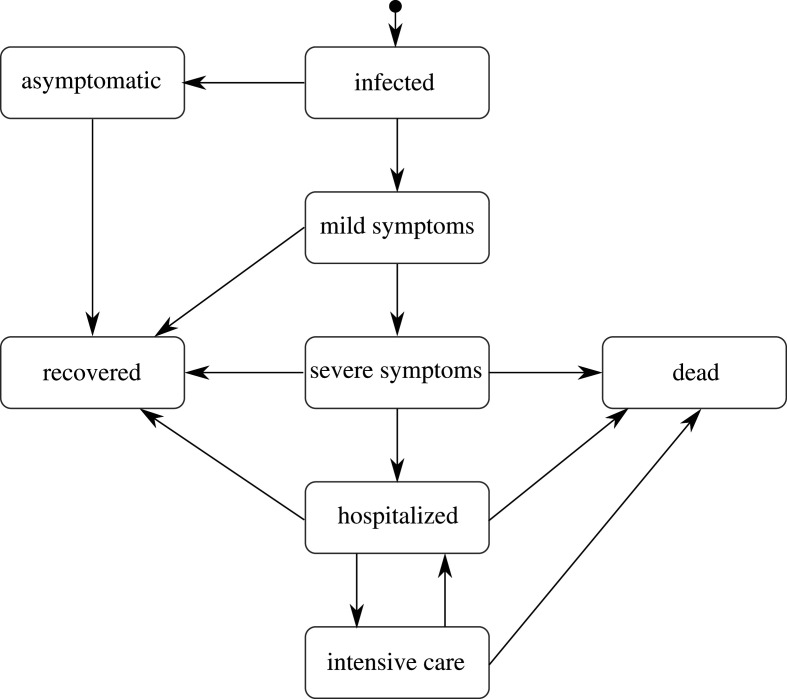
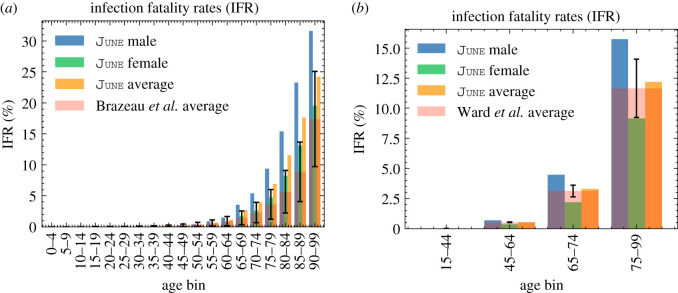
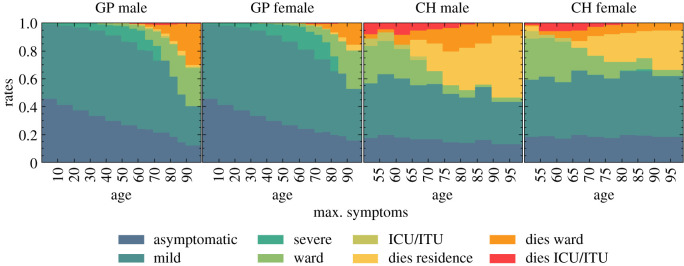
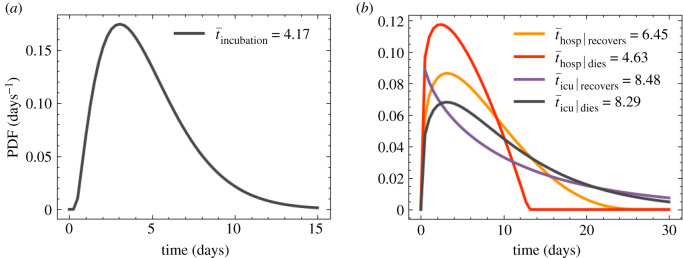
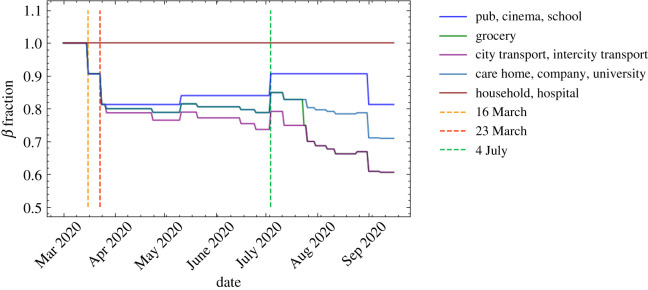
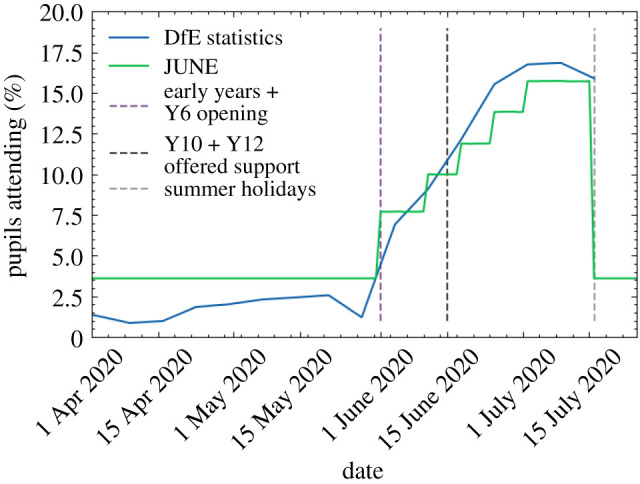
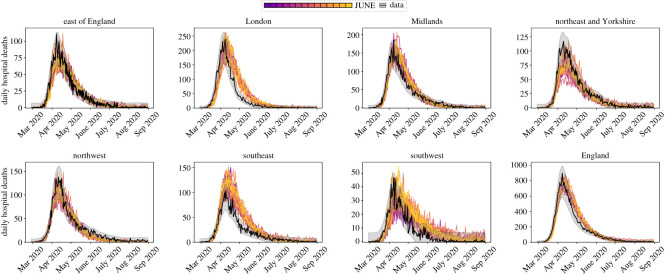
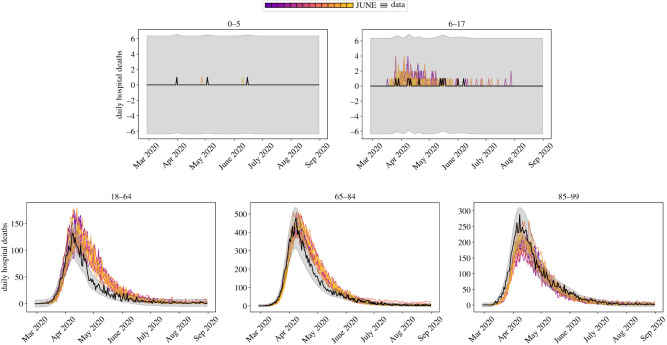
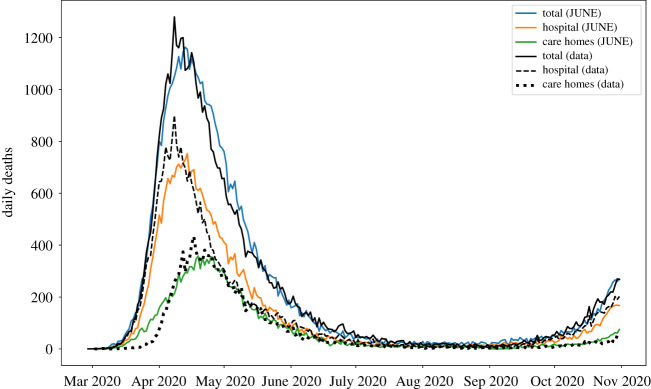
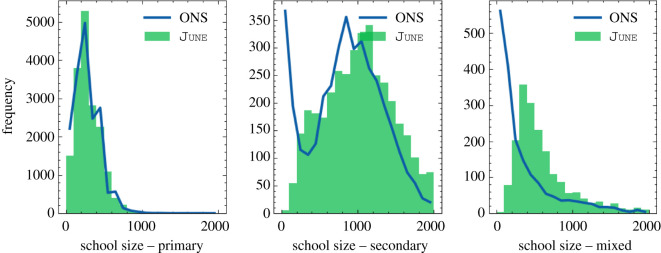
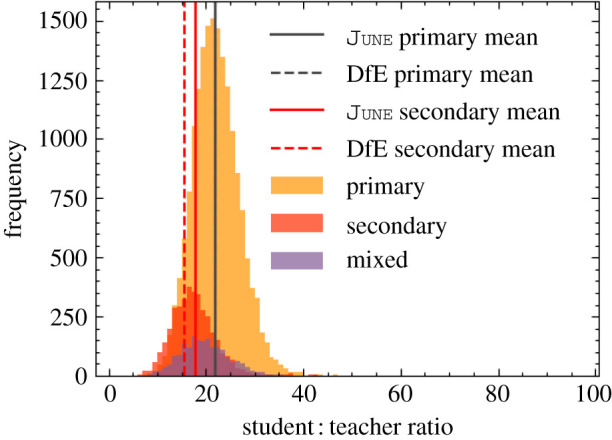
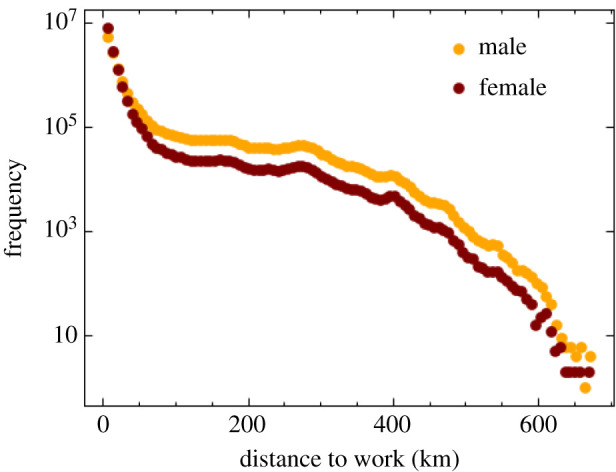
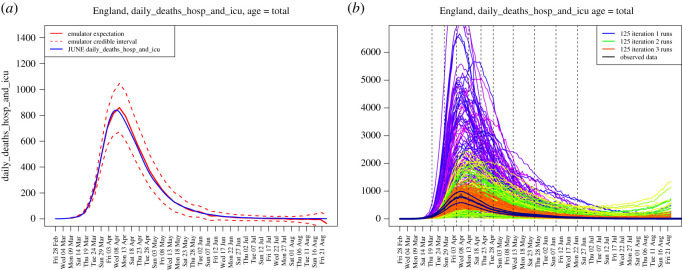
We introduce June, an open-source framework for the detailed simulation of epidemics on the basis of social interactions in a virtual population constructed from geographically granular census data, reflecting age, sex, ethnicity and socio-economic indicators. Interactions between individuals are modelled in groups of various sizes and properties, such as households, schools and workplaces, and other social activities using social mixing matrices. June provides a suite of flexible parametrizations that describe infectious diseases, how they are transmitted and affect contaminated individuals. In this paper, we apply June to the specific case of modelling the spread of COVID-19 in England. We discuss the quality of initial model outputs which reproduce reported hospital admission and mortality statistics at national and regional levels as well as by age strata.
Keywords: individual-based model; infectious disease; simulation.
© 2021 The Authors.
Figures
References
LinkOut - more resources
Full Text Sources