

Combined bone scintigraphy and fluorocholine PET/computed tomography predicts response to radium-223 therapy in patients with prostate cancer
- PMID: 34295537
- PMCID: PMC8288237
- DOI: 10.2144/fsoa-2021-0053
Combined bone scintigraphy and fluorocholine PET/computed tomography predicts response to radium-223 therapy in patients with prostate cancer
Abstract
Aim: To assess the value of bone scintigraphy and 18F-fluorocholine PET/computed tomography (CT) in predicting outcome in patients with prostate cancer and bone metastases treated with 223radium.
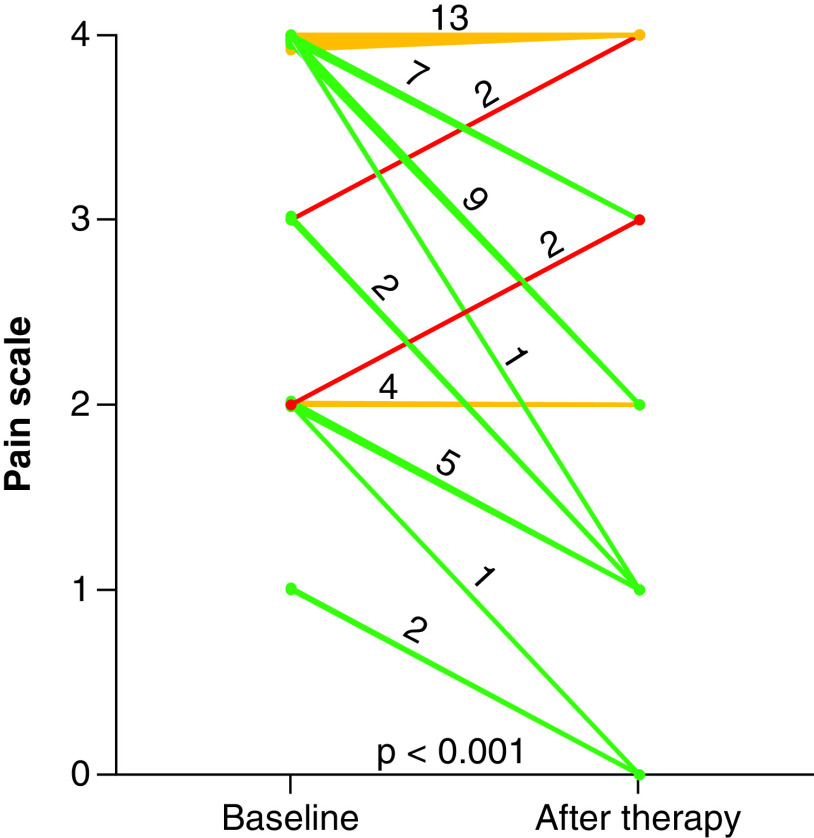
Materials & methods: Retrospective analysis of 48 patients that underwent 223radium therapy. End points were pain relief and overall survival.
Results: After therapy, pain relief was observed in 27 patients. Patients without pain relief had more bone lesions at PET/CT than at bone scintigraphy (pretherapy imaging mismatch). In 39 patients who completed treatment protocol, post-therapy alkaline phosphatase and pretherapy imaging mismatch were independent predictors of poor overall survival.
Conclusion: Patients with more lesions at 18F-fluorocholine PET/CT than at bone scintigraphy had a poor prognosis. The combined imaging approach could be useful to predict outcome after 223radium therapy.
Keywords: 18F-fluorocholine PET/CT outcome; 223radium; bone scintigraphy; prostate cancer.
© 2021 Alberto Cuocolo.
Conflict of interest statement
Financial & competing interests disclosure The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. No writing assistance was utilized in the production of this manuscript.
Figures



References
-
- Culp MB, Soerjomataram I, Efstathiou JA, Bray F, Jemal A. Recent global patterns in prostate cancer incidence and mortality rates. Eur. Urol. 77(1), 38–52 (2020). - PubMed
-
•• Basic clinical investigation.
-
- Rubens RD. Bone metastases – incidence and complications. : Cancer and the Skeleton. Mundy GR (). Martin Dunitz, London, 33–42 (2000).
-
- Fitzpatrick JM, Bellmunt J, Fizazi K et al. Optimal management of metastatic castration-resistant prostate cancer: highlights from a European Expert Consensus Panel. Eur. J. Cancer 50(9), 1617–1627 (2014). - PubMed
-
- Seruga B, Ocana A, Tannock IF. Drug resistance in metastatic castration-resistant prostate cancer. Nat. Rev. Clin. Oncol. 8(1), 12–23 (2011). - PubMed
-
- Nuhn P, De Bono JS, Fizazi K et al. Update on systemic prostate cancer therapies: management of metastatic castration-resistant prostate cancer in the era of precision oncology. Eur. Urol. 75(1), 88–99 (2019). - PubMed
LinkOut - more resources
Full Text Sources