

Alternaria chartarum sclerokeratouveitis: A new fungus cause
- PMID: 34295628
- PMCID: PMC8259522
- DOI: 10.4103/tjo.tjo_17_19
Alternaria chartarum sclerokeratouveitis: A new fungus cause
Abstract
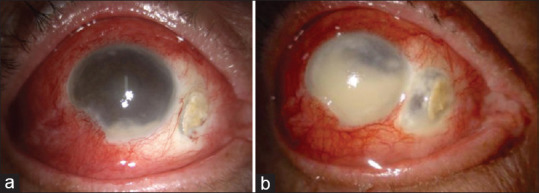
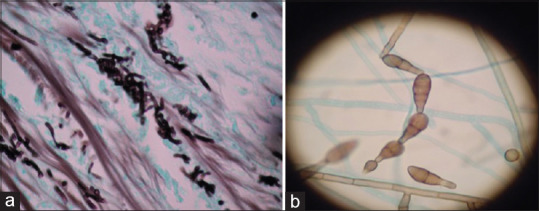
We report a case of Alternaria chartarum sclerokeratouveitis with an unfavorable response to treatment. To the best of our knowledge, there are no previous reports of this fungus invading the sclera. A 68-year-old diabetic farmer male patient presented with a 3-week history of pain and redness and a decrease in visual acuity occurring 5 days before admittance in the right eye. Examination revealed severe mixed hyperemia and a scleral calcified plaque with a surrounding area of ischemia and lysis. The cornea showed diffuse infiltrates, stromal edema, and hypopyon. Initial scrapings were negative, and empiric antibiotics were started. After a fungus was reported, topical and systemic antifungals were initiated, but there was no clinical response. The eye was enucleated. A slow-growing fungus A. chartarum, resistant to voriconazole, was isolated. Fungal etiology must be kept in mind when dealing with infectious scleritis. Despite treatment, the outcome of this case was unfavorable due to the slow-growing nature of the fungus and this strain's resistance to voriconazole.
Keywords: Alternaria chartarum; fungus; sclerokeratouveitis.
Copyright: © 2020 Taiwan J Ophthalmol.
Conflict of interest statement
The authors declare that there are no conflicts of interests of this paper.
Figures
References
-
- Hodson KL, Galor A, Karp CL, Davis JL, Albini TA, Perez VL, et al. Epidemiology and visual outcomes in patients with infectious scleritis. Cornea. 2013;32:466–72. - PubMed
-
- Ho YF, Yeh LK, Tan HY, Chen HC, Chen YF, Lin HC, et al. Infectious scleritis in Taiwan-a 10-year review in a tertiary-care hospital. Cornea. 2014;33:838–43. - PubMed
-
- Pujol I, Aguilar C, Gené J, Guarro J. In vitro antifungal susceptibility of Alternaria spp.and Ulocladium spp. J Antimicrob Chemother. 2000;46:337. - PubMed
Publication types
LinkOut - more resources
Full Text Sources