

Big Data, Data Science, and Causal Inference: A Primer for Clinicians
- PMID: 34295910
- PMCID: PMC8290071
- DOI: 10.3389/fmed.2021.678047
Big Data, Data Science, and Causal Inference: A Primer for Clinicians
Abstract
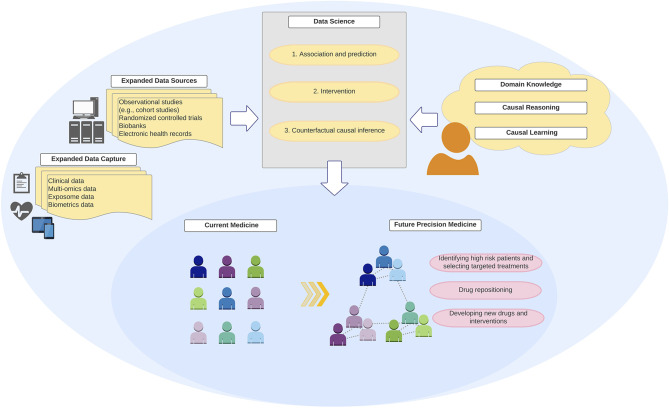
Clinicians handle a growing amount of clinical, biometric, and biomarker data. In this "big data" era, there is an emerging faith that the answer to all clinical and scientific questions reside in "big data" and that data will transform medicine into precision medicine. However, data by themselves are useless. It is the algorithms encoding causal reasoning and domain (e.g., clinical and biological) knowledge that prove transformative. The recent introduction of (health) data science presents an opportunity to re-think this data-centric view. For example, while precision medicine seeks to provide the right prevention and treatment strategy to the right patients at the right time, its realization cannot be achieved by algorithms that operate exclusively in data-driven prediction modes, as do most machine learning algorithms. Better understanding of data science and its tasks is vital to interpret findings and translate new discoveries into clinical practice. In this review, we first discuss the principles and major tasks of data science by organizing it into three defining tasks: (1) association and prediction, (2) intervention, and (3) counterfactual causal inference. Second, we review commonly-used data science tools with examples in the medical literature. Lastly, we outline current challenges and future directions in the fields of medicine, elaborating on how data science can enhance clinical effectiveness and inform medical practice. As machine learning algorithms become ubiquitous tools to handle quantitatively "big data," their integration with causal reasoning and domain knowledge is instrumental to qualitatively transform medicine, which will, in turn, improve health outcomes of patients.
Keywords: big data; causal inference; data science; machine learning; the ladder of causation.
Copyright © 2021 Raita, Camargo, Liang and Hasegawa.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Pearl J. The seven tools of causal inference, with reflections on machine learning. Commun ACM. (2019) 62:54–60. 10.1145/3241036 - DOI
-
- Donoho D. 50 Years of data science. J Comput Graph Stat. (2017) 26:745–66. 10.1080/10618600.2017.1384734 - DOI
-
- Fisher RA. Statistical Methods for Research Workers. 1st ed. Edinburgh: Oliver and Boyd: (1925).
Publication types
LinkOut - more resources
Full Text Sources
Research Materials