

Multimodal Mapping of the Tumor and Peripheral Blood Immune Landscape in Human Pancreatic Cancer
- PMID: 34296197
- PMCID: PMC8294470
- DOI: 10.1038/s43018-020-00121-4
Multimodal Mapping of the Tumor and Peripheral Blood Immune Landscape in Human Pancreatic Cancer
Abstract
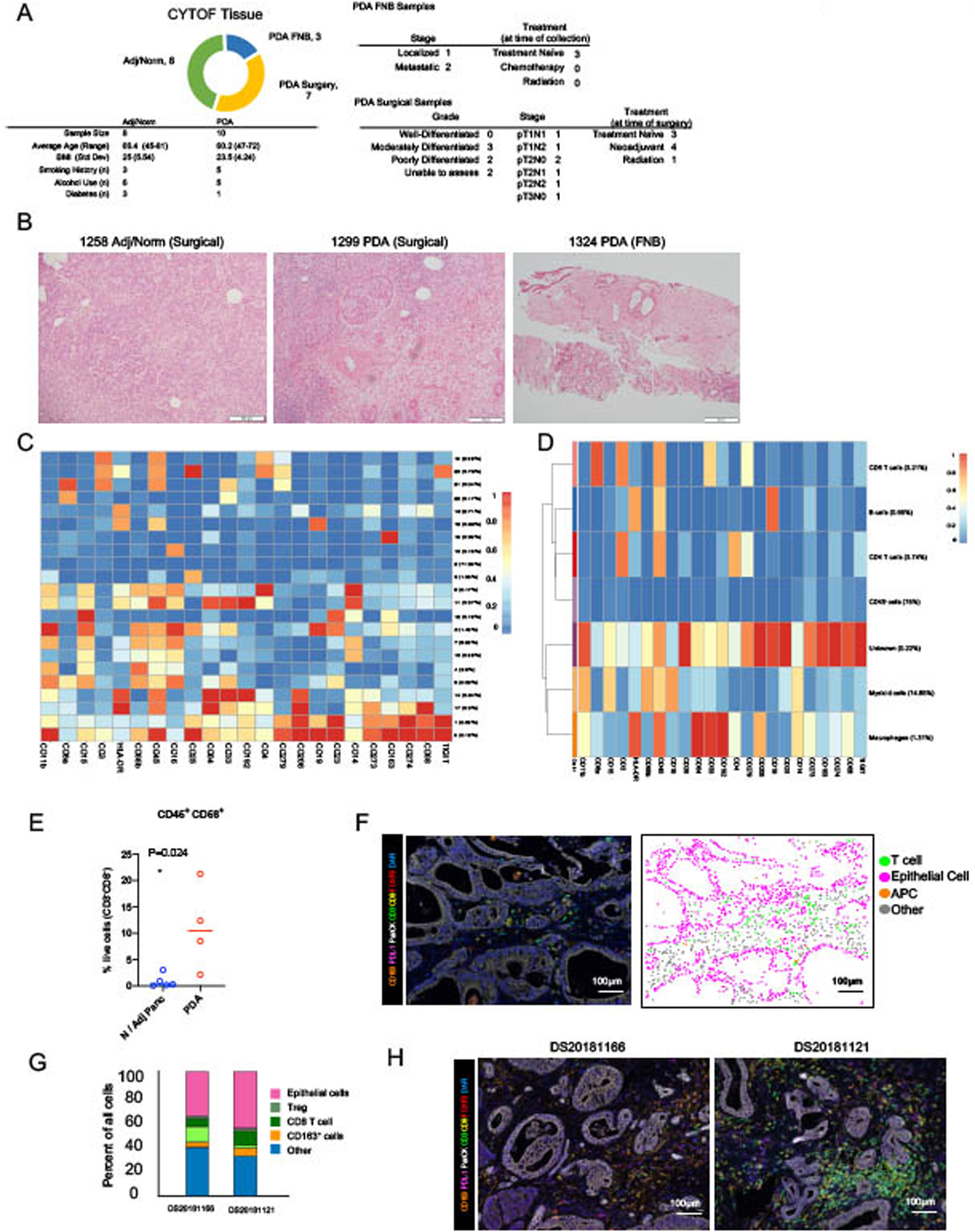
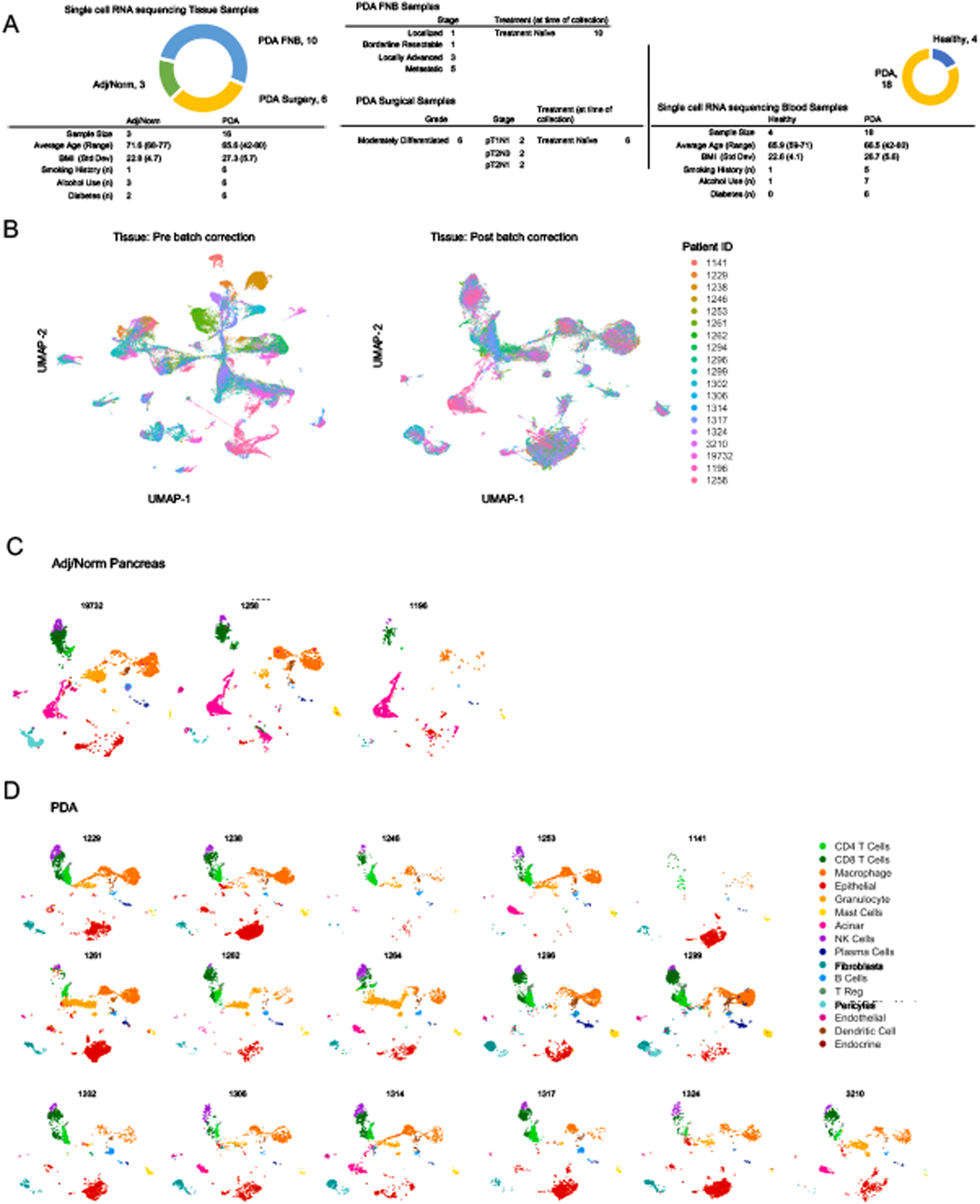
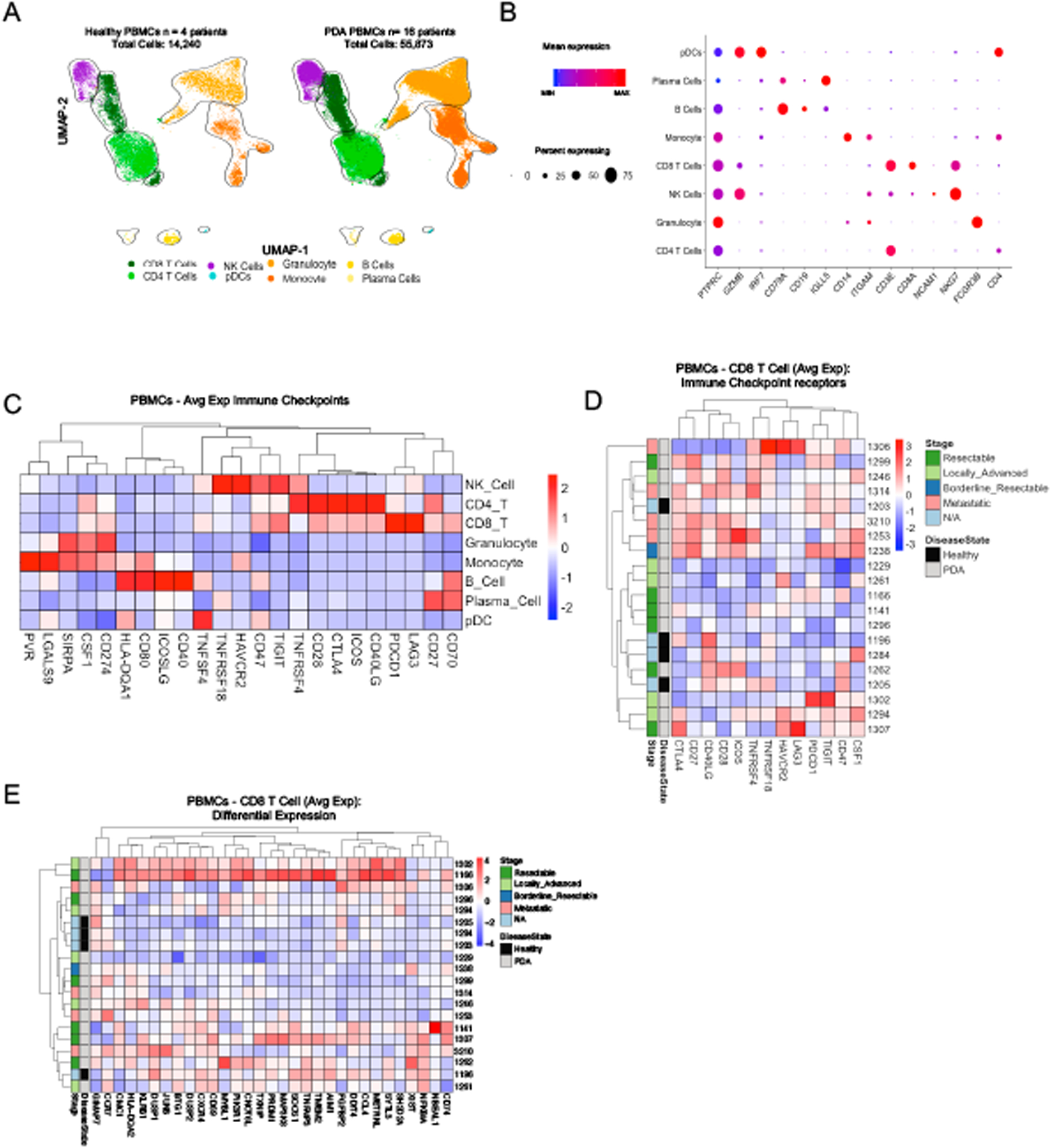
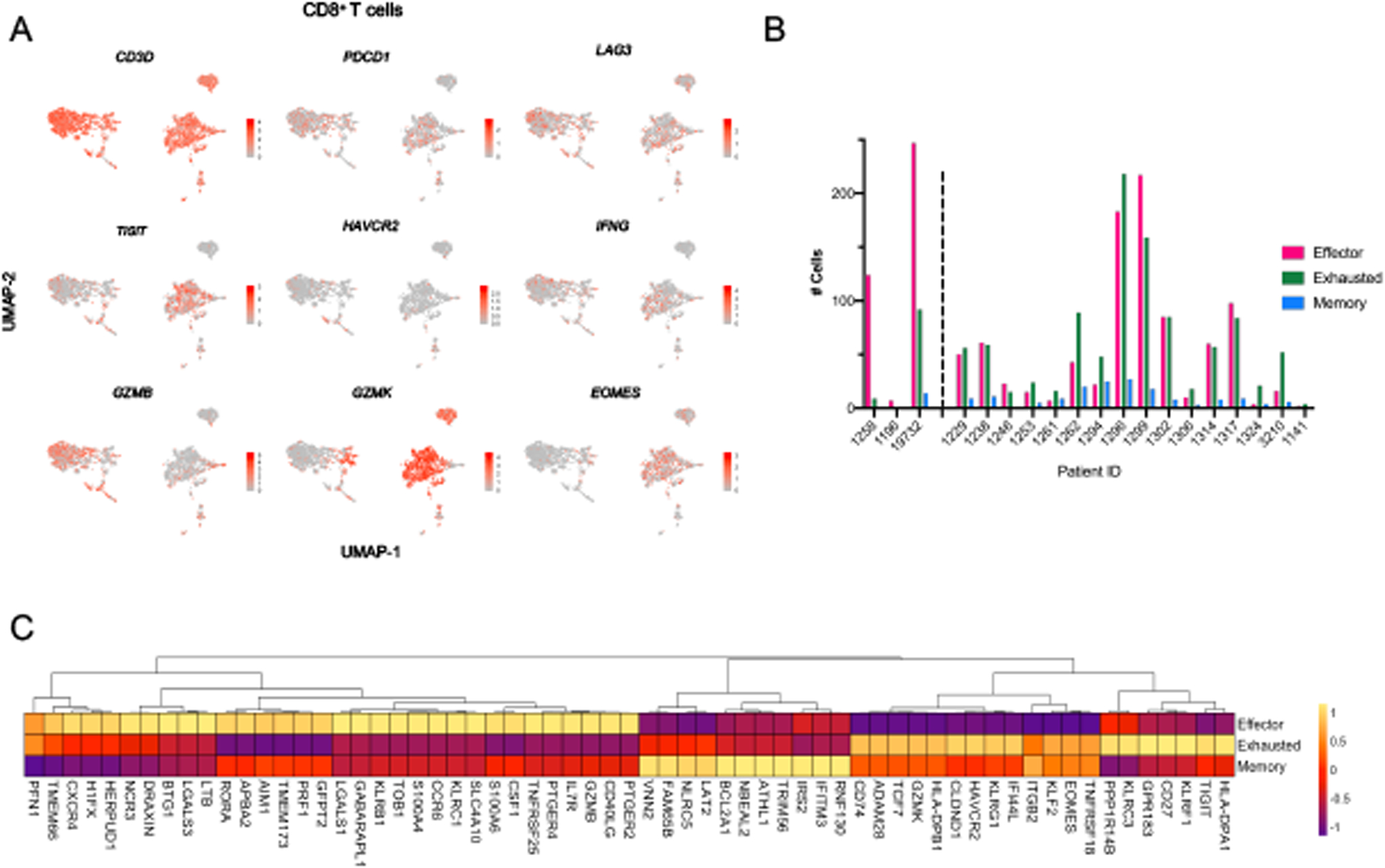
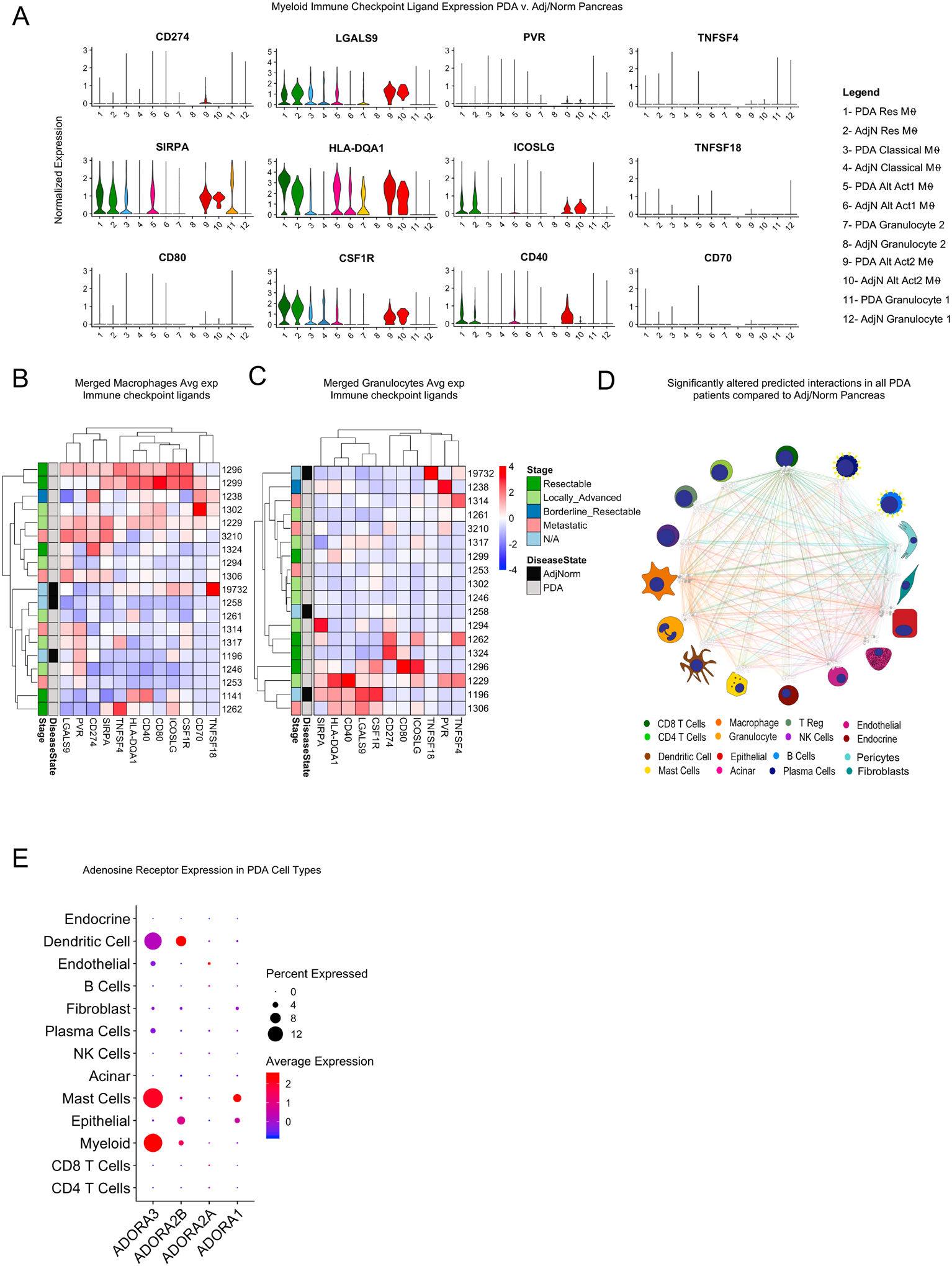
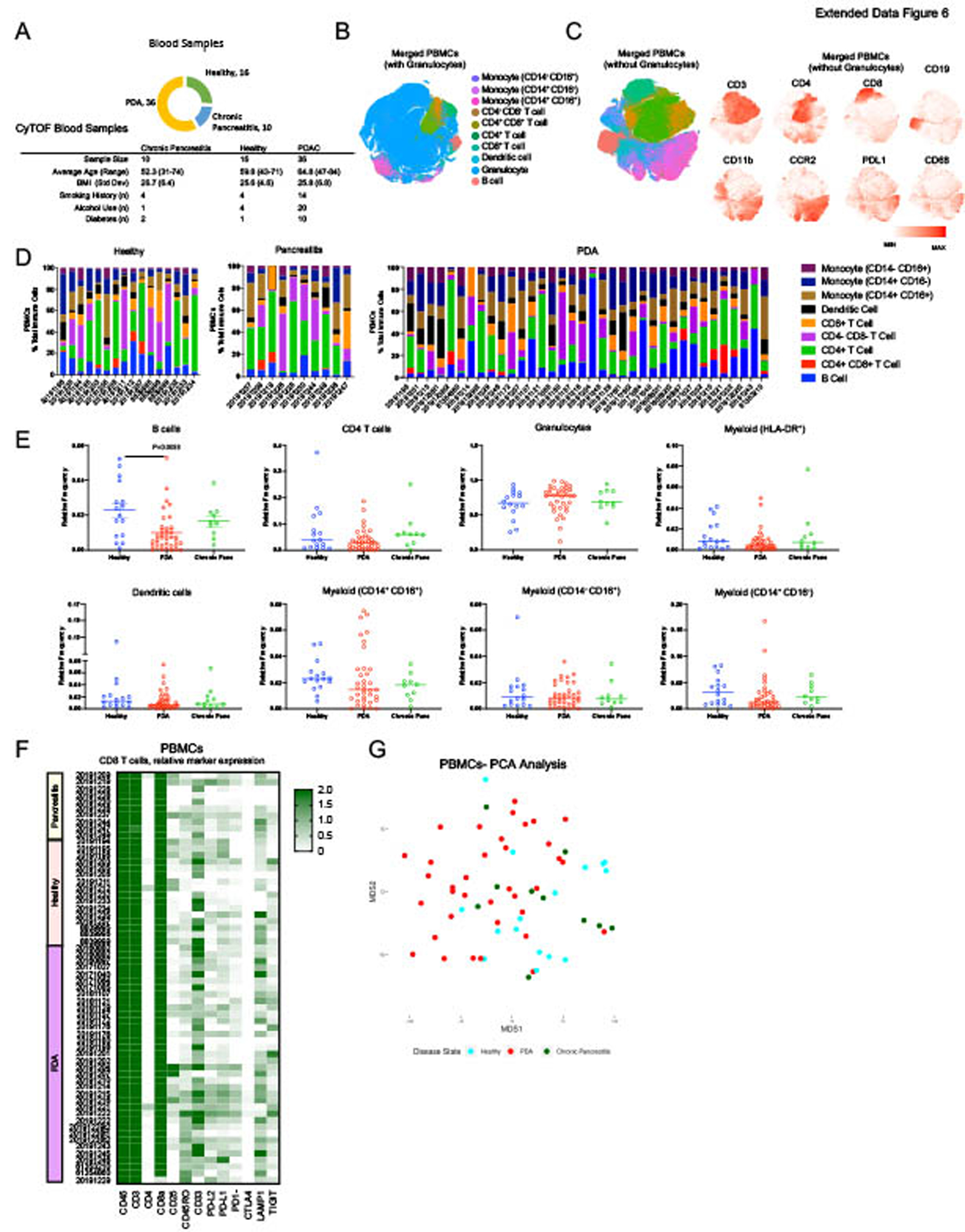
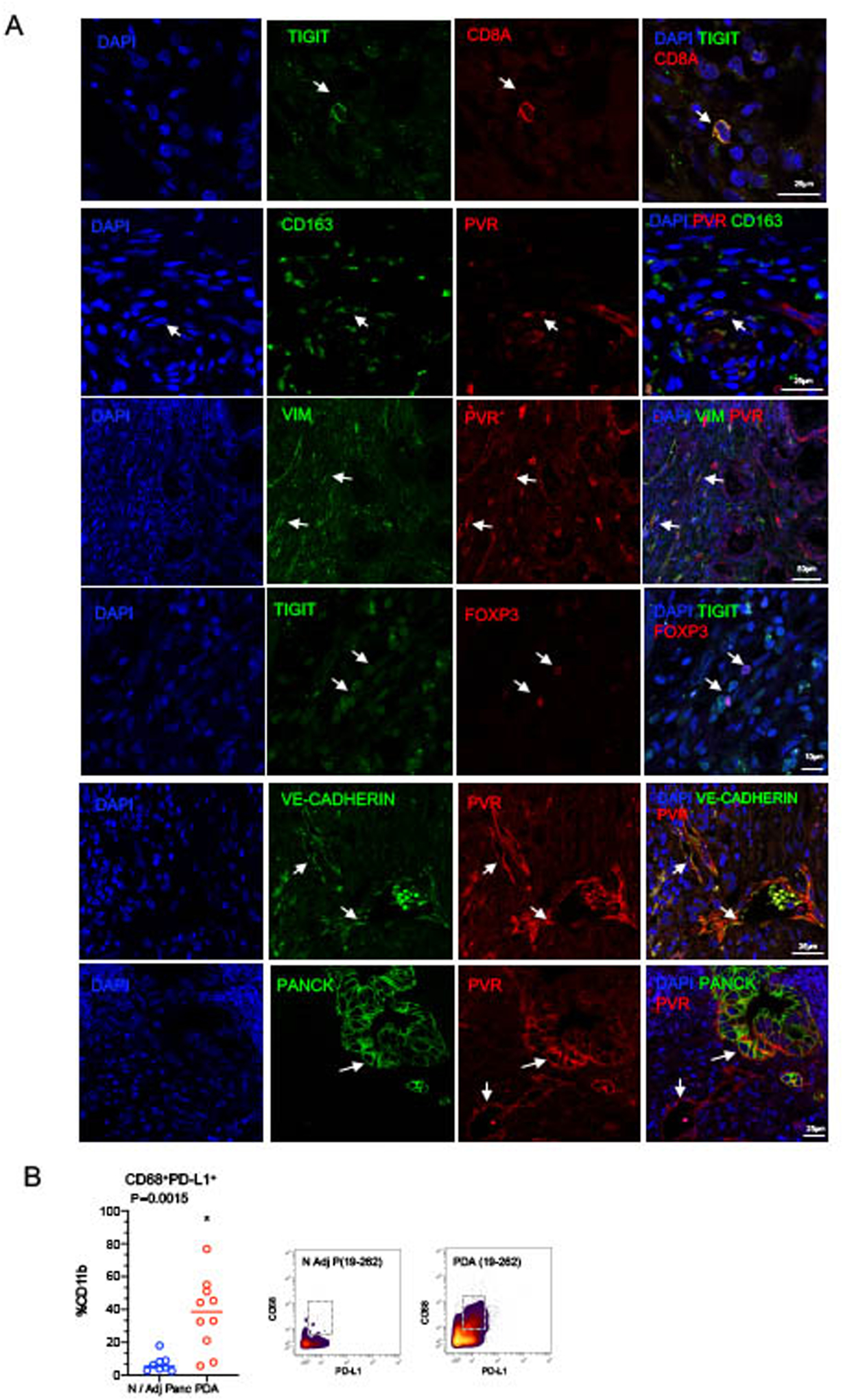
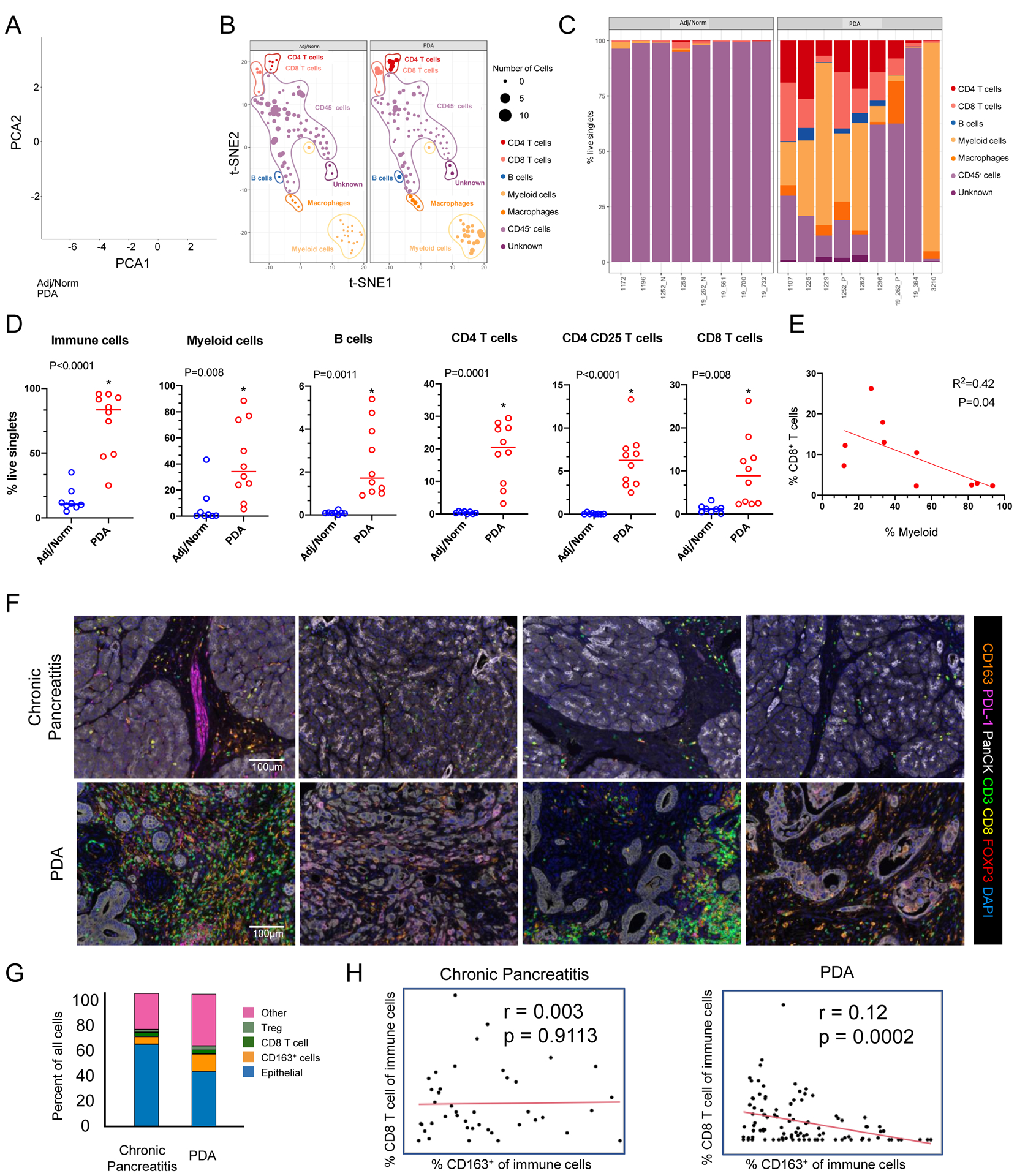
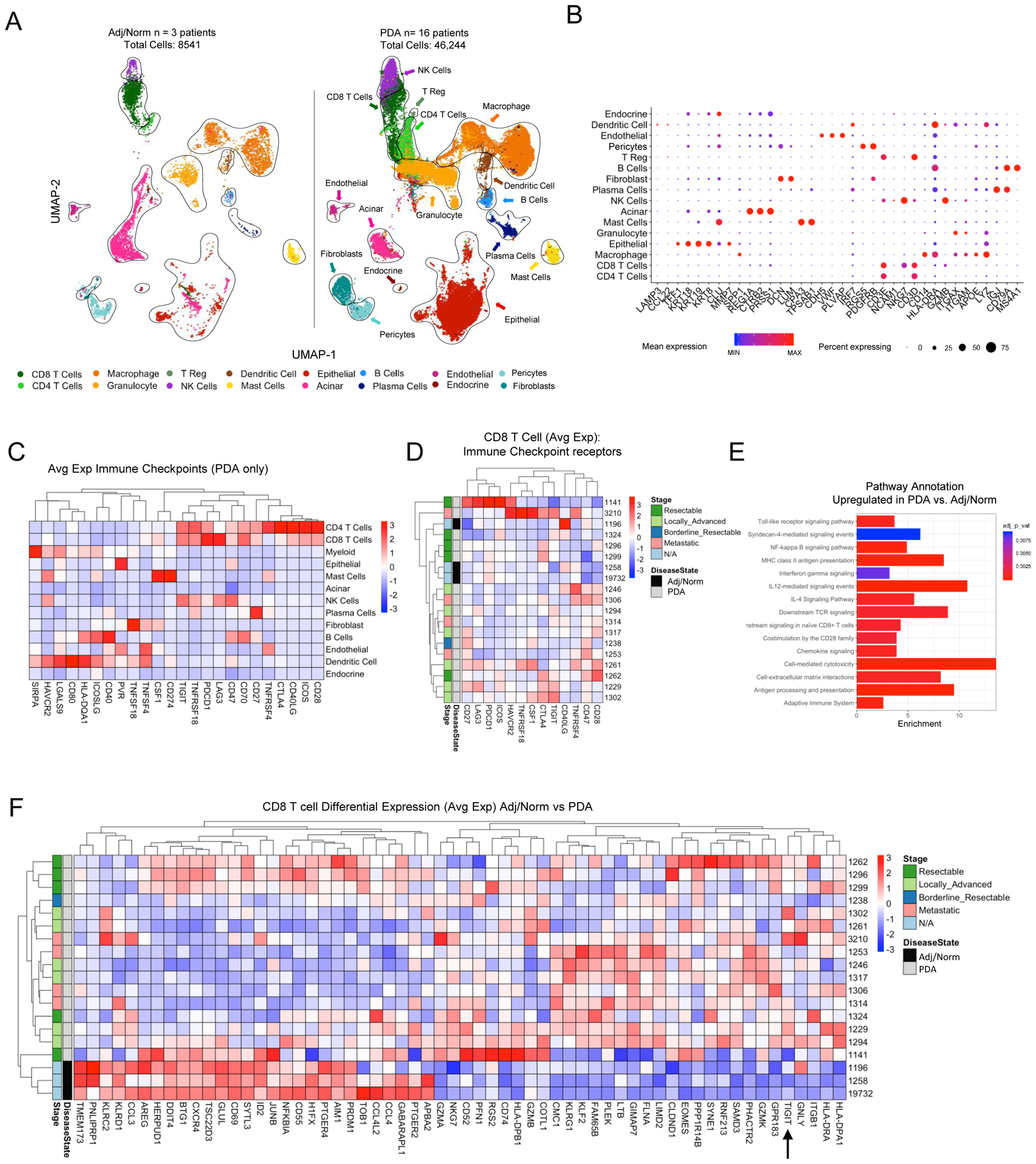
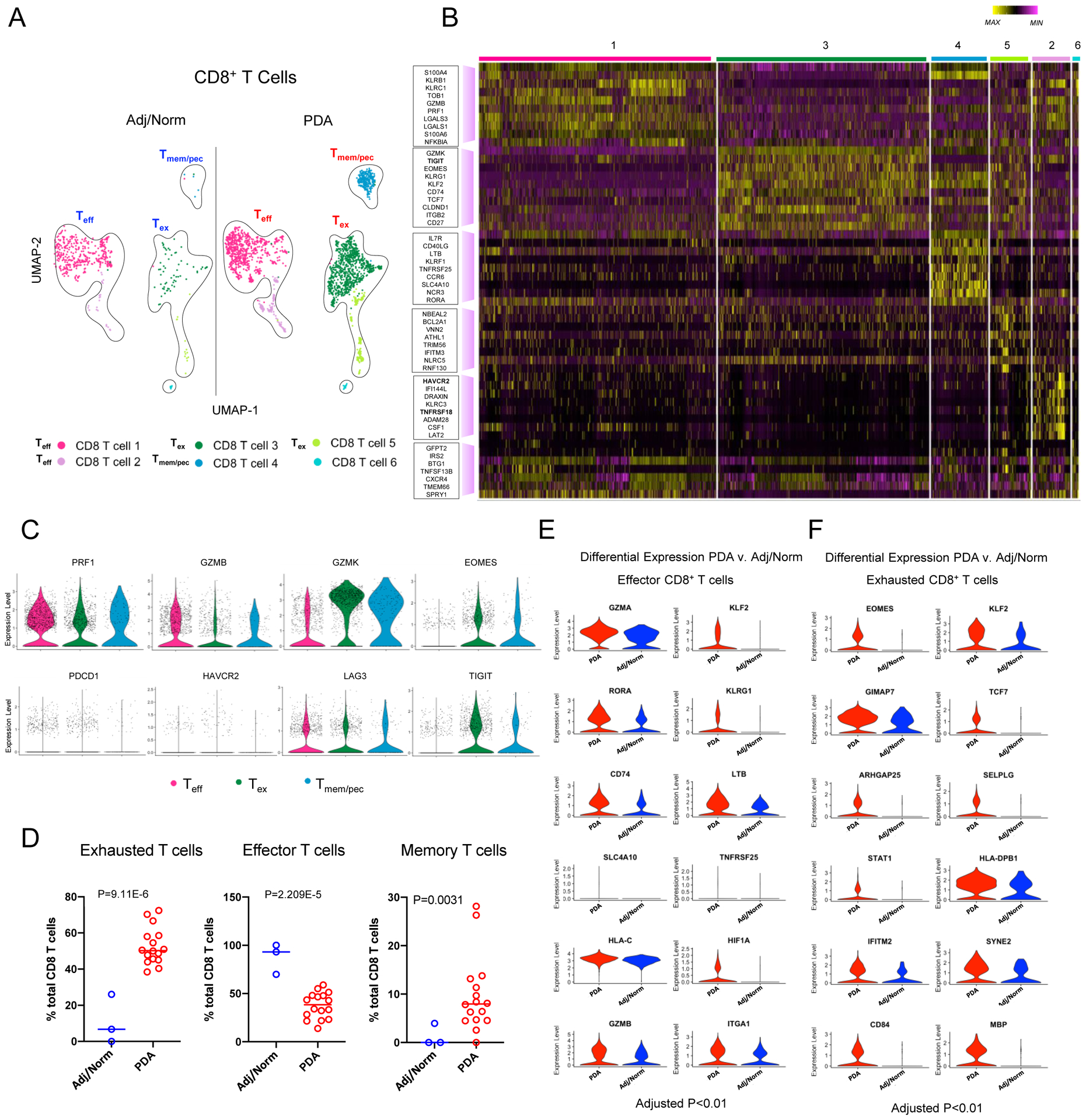
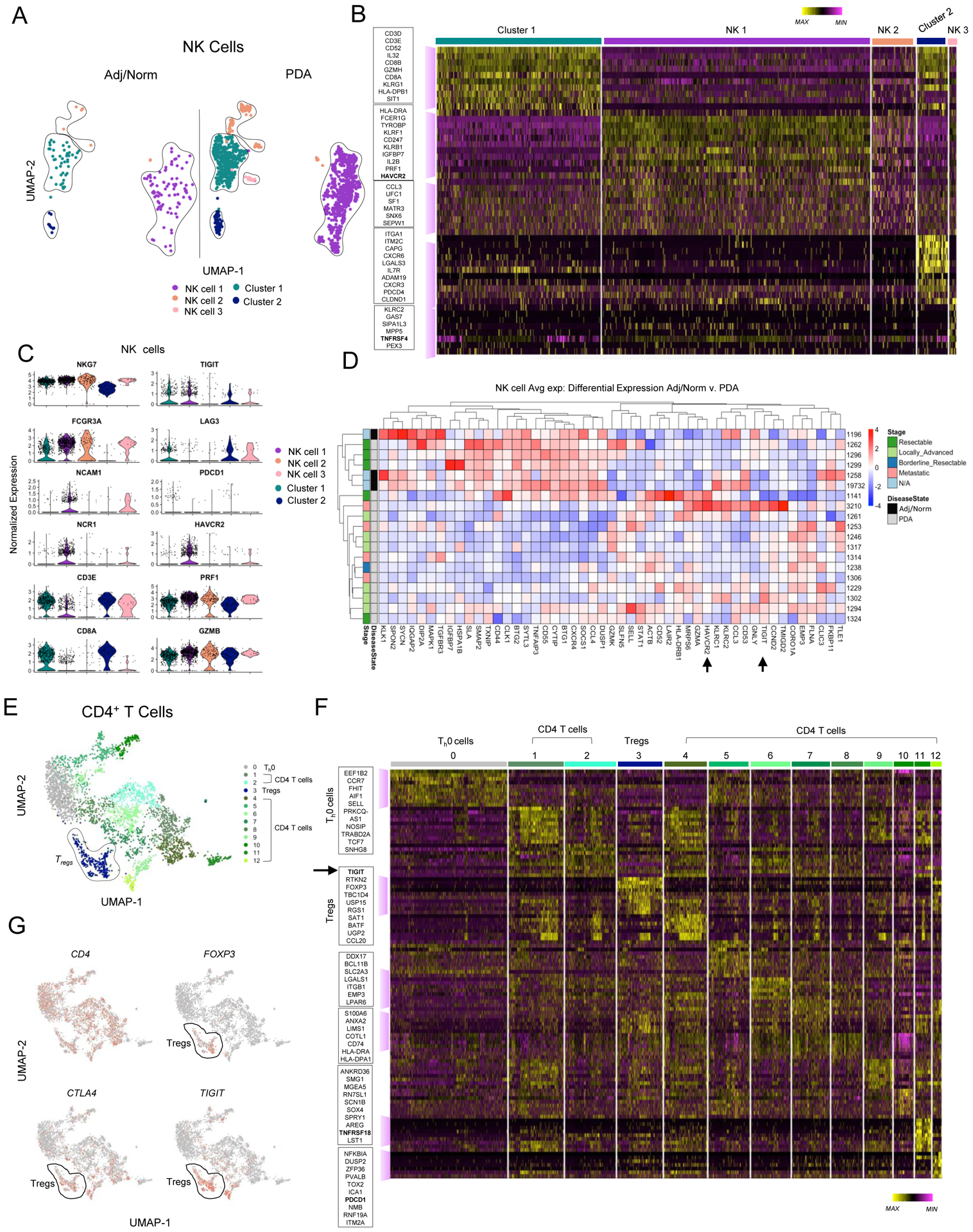
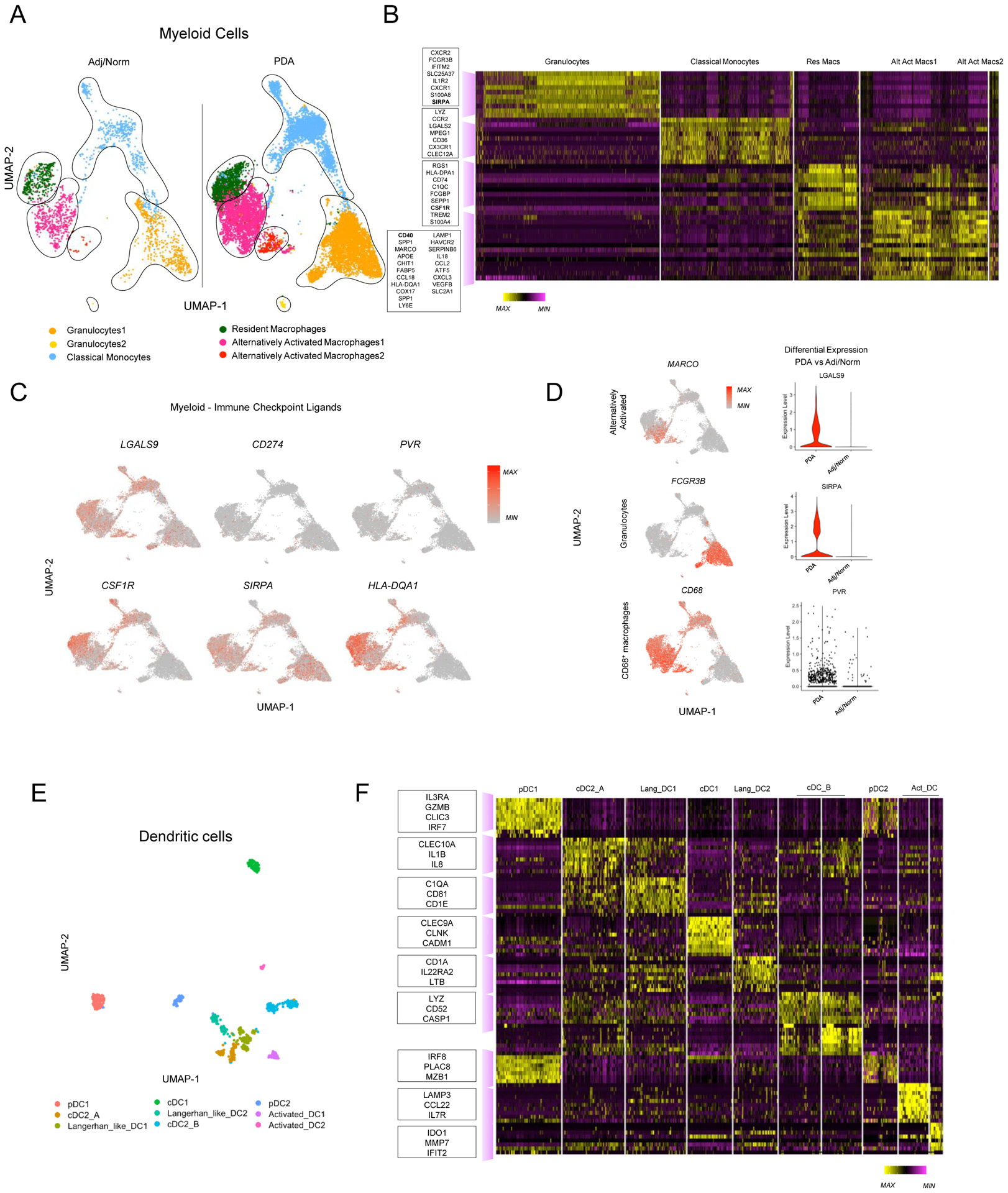
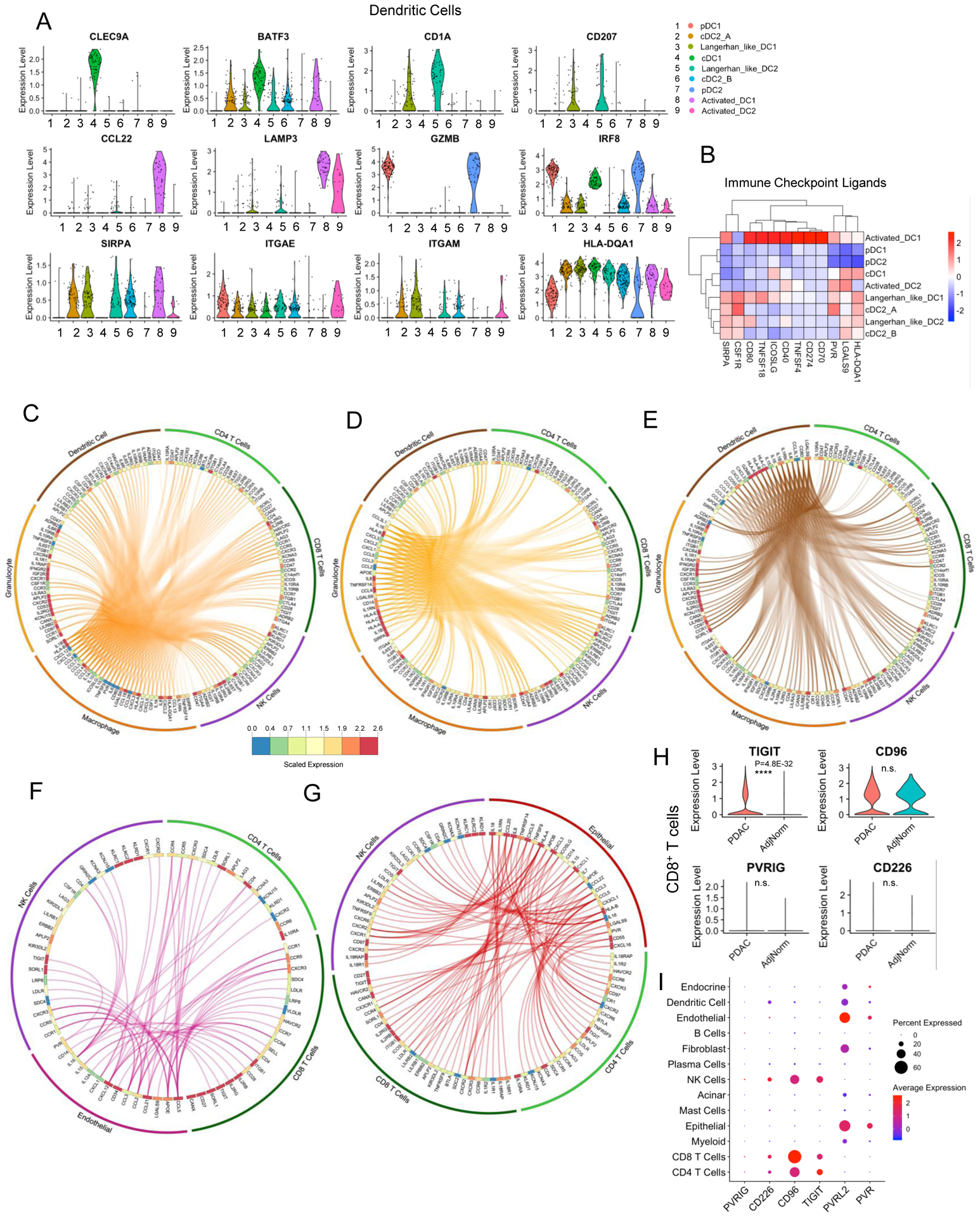
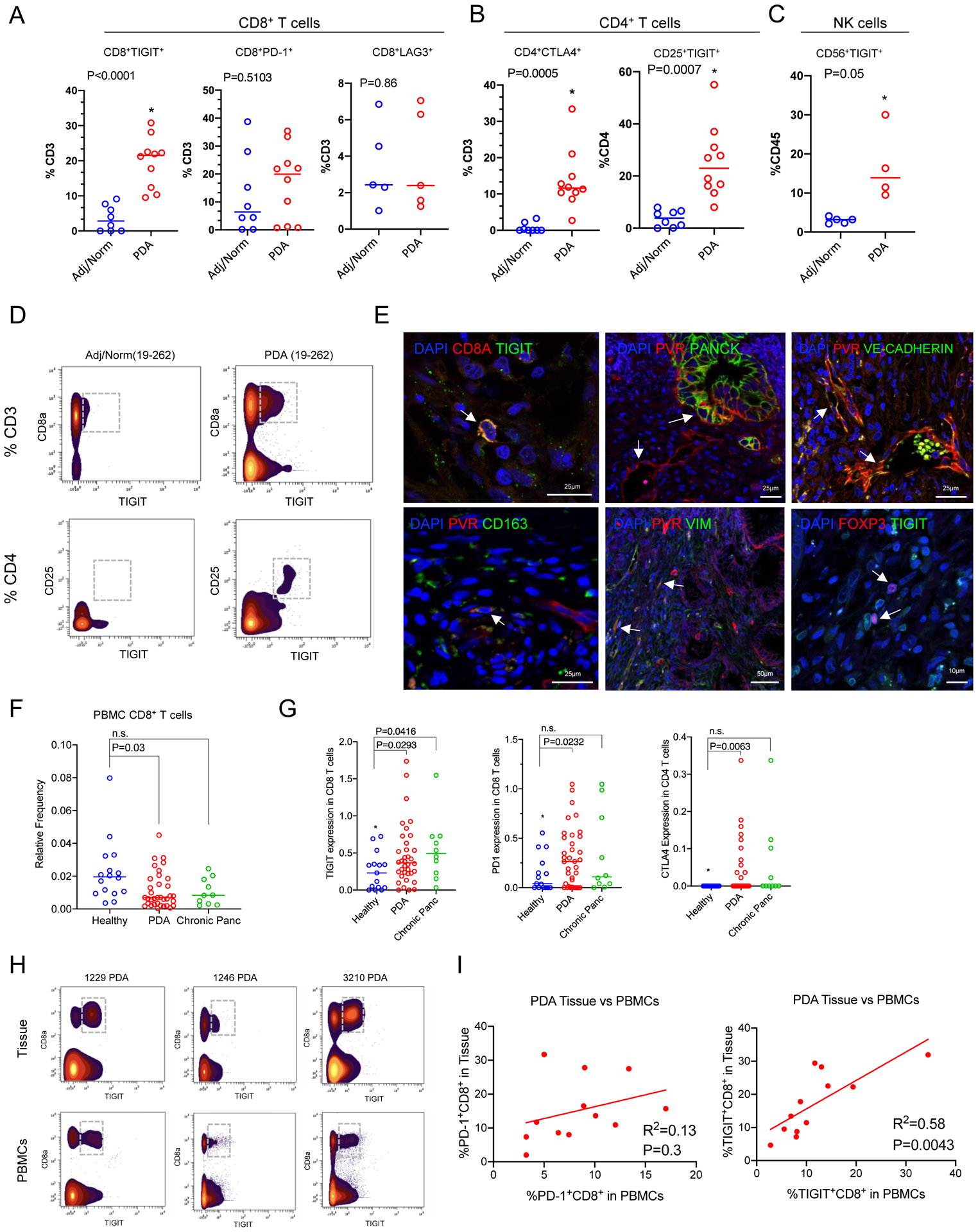
Pancreatic ductal adenocarcinoma (PDA) is characterized by an immune-suppressive tumor microenvironment that renders it largely refractory to immunotherapy. We implemented a multimodal analysis approach to elucidate the immune landscape in PDA. Using a combination of CyTOF, single-cell RNA sequencing, and multiplex immunohistochemistry on patient tumors, matched blood, and non-malignant samples, we uncovered a complex network of immune-suppressive cellular interactions. These experiments revealed heterogeneous expression of immune checkpoint receptors in individual patient's T cells and increased markers of CD8+ T cell dysfunction in advanced disease stage. Tumor-infiltrating CD8+ T cells had an increased proportion of cells expressing an exhausted expression profile that included upregulation of the immune checkpoint TIGIT, a finding that we validated at the protein level. Our findings point to a profound alteration of the immune landscape of tumors, and to patient-specific immune changes that should be taken into account as combination immunotherapy becomes available for pancreatic cancer.
Keywords: CD8+ T cells; Single-cell RNA sequencing; TIGIT; immune checkpoints; pancreatic cancer; tumor immunology.
Conflict of interest statement
Competing interests: The authors have declared that no conflict of interest exists.
Figures
References
References and Notes:
-
- RStudio Team (2015). RStudio: Integrated Development for R. RStudio, Inc, Boston, MA: URL http://www.rstudio.com/.
-
- R Core Team (2017). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/.
References
-
- Balli D, et al., Immune Cytolytic Activity Stratifies Molecular Subsets of Human Pancreatic Cancer. Clin Cancer Res, 2017. 23(12): p. 3129–3138. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 CA198074/CA/NCI NIH HHS/United States
- P30 CA046592/CA/NCI NIH HHS/United States
- T32 GM113900/GM/NIGMS NIH HHS/United States
- R01 CA151588/CA/NCI NIH HHS/United States
- R01 CA248160/CA/NCI NIH HHS/United States
- R37 CA214955/CA/NCI NIH HHS/United States
- U01 CA224145/CA/NCI NIH HHS/United States
- I01 BX005777/BX/BLRD VA/United States
- T32 CA009676/CA/NCI NIH HHS/United States
- P30 DK034933/DK/NIDDK NIH HHS/United States
- K08 CA201581/CA/NCI NIH HHS/United States
- R01 CA247516/CA/NCI NIH HHS/United States
- T32 DK094775/DK/NIDDK NIH HHS/United States
- R37 CA237421/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
