

Prognostic Impact of Resection Margin Status in Distal Pancreatectomy for Ductal Adenocarcinoma
- PMID: 34296358
- PMCID: PMC8677636
- DOI: 10.1245/s10434-021-10464-6
Prognostic Impact of Resection Margin Status in Distal Pancreatectomy for Ductal Adenocarcinoma
Abstract
Background: Resection margin status is considered one of the few surgeon-controlled parameters affecting prognosis in pancreatic ductal adenocarcinoma (PDAC). While studies mostly focus on resection margins in pancreatoduodenectomy, little is known about their role in distal pancreatectomy (DP). This study aimed to investigate resection margins in DP for PDAC.
Methods: Patients who underwent DP for PDAC between October 2004 and February 2020 were included (n = 124). Resection margins and associated parameters were studied in two consecutive time periods during which different pathology examination protocols were used: non-standardized (period 1: 2004-2014) and standardized (period 2: 2015-2020). Microscopic margin involvement (R1) was defined as ≤1 mm clearance.
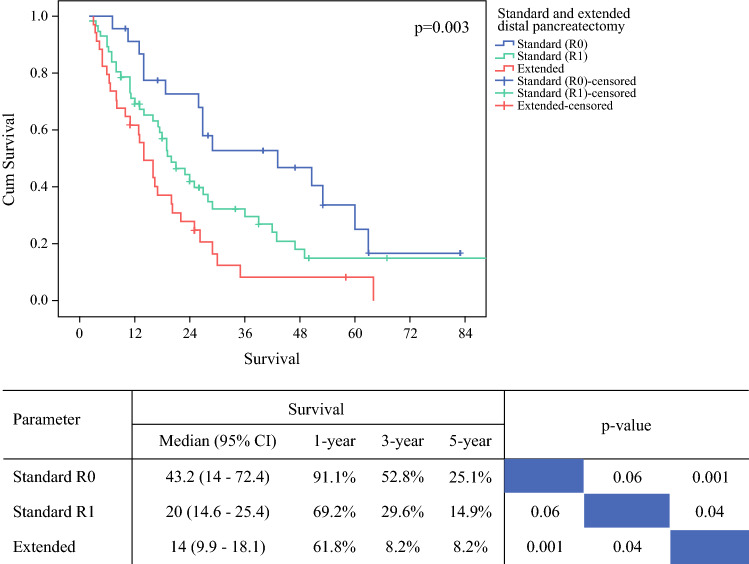
Results: Laparoscopic and open resections were performed in 117 (94.4%) and 7 (5.6%) patients, respectively. The R1 rate for the entire cohort was 73.4%, increasing from 60.4% in period 1 to 83.1% in period 2 (p = 0.005). A significantly higher R1 rate was observed for the posterior margin (35.8 vs. 70.4%, p < 0.001) and anterior pancreatic surface (based on a 0 mm clearance; 18.9 vs. 35.4%, p = 0.045). Pathology examination period, poorly differentiated PDAC, and vascular invasion were associated with R1 in the multivariable model. Extended DP, positive anterior pancreatic surface, lymph node ratio, perineural invasion, and adjuvant chemotherapy, but not R1, were significant prognostic factors for overall survival in the entire cohort.
Conclusions: Pathology examination is a key determinant of resection margin status following DP for PDAC. A high R1 rate is to be expected when pathology examination is meticulous and standardized. Involvement of the anterior pancreatic surface affects prognosis.
© 2021. The Author(s).
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
