

Spontaneous intracranial hypotension: diagnostic and therapeutic workup
- PMID: 34297176
- PMCID: PMC8528761
- DOI: 10.1007/s00234-021-02766-z
Spontaneous intracranial hypotension: diagnostic and therapeutic workup
Abstract
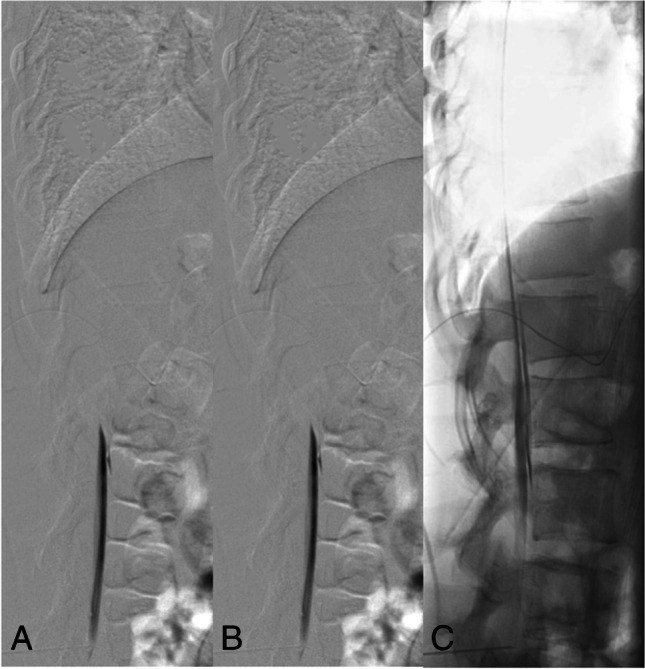
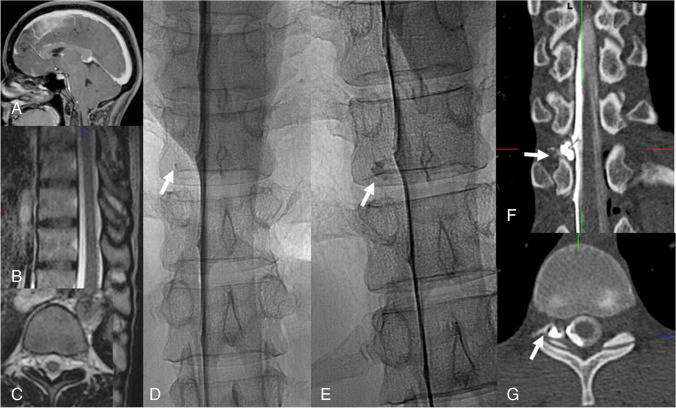
Spontaneous intracranial hypotension (SIH) is an orthostatic headache syndrome with typical MRI findings among which engorgement of the venous sinuses, pachymeningeal enhancement, and effacement of the suprasellar cistern have the highest diagnostic sensitivity. SIH is in almost all cases caused by spinal CSF leaks. Spinal MRI scans showing so-called spinal longitudinal extradural fluid (SLEC) are suggestive of ventral dural tears (type 1 leak) which are located with prone dynamic (digital subtraction) myelography. As around half of the ventral dural tears are located in the upper thoracic spine, additional prone dynamic CT myelography is often needed. Leaking nerve root sleeves typically associated with meningeal diverticulae (type 2 leaks) and CSF-venous fistulas (type 3 leaks) are proven via lateral decubitus dynamic digital subtraction or CT myelography: type 2 leaks are SLEC-positive if the tear is proximal and SLEC-negative if it is distal, and type 3 leaks are always SLEC-negative. Although 30-70% of SIH patients show marked improvement following epidural blood patches applied via various techniques definite cure mostly requires surgical closure of ventral dural tears and surgical ligations of leaking nerve root sleeves associated with meningeal diverticulae or CSF-venous fistulas. For the latter, transvenous embolization with liquid embolic agents via the azygos vein system is a novel and valuable therapeutic alternative.
Keywords: CSF-venous fistula; Lateral decubitus myelography; Spontaneous intracranial hypotension.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures




References
-
- Headache Classification Committee of the International Headache Society (IHS) (2018) The international classification of headache disorders, 3rd edition. Cephalalgia 38:1–211 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
