

The synchronicity of COVID-19 disparities: Statewide epidemiologic trends in SARS-CoV-2 morbidity, hospitalization, and mortality among racial minorities and in rural America
- PMID: 34297747
- PMCID: PMC8301667
- DOI: 10.1371/journal.pone.0255063
The synchronicity of COVID-19 disparities: Statewide epidemiologic trends in SARS-CoV-2 morbidity, hospitalization, and mortality among racial minorities and in rural America
Abstract
Background: Early studies on COVID-19 identified unequal patterns in hospitalization and mortality in urban environments for racial and ethnic minorities. These studies were primarily single center observational studies conducted within the first few weeks or months of the pandemic. We sought to examine trends in COVID-19 morbidity, hospitalization, and mortality over time for minority and rural populations, especially during the U.S. fall surge.
Methods: Data were extracted from a statewide cohort of all adult residents in Indiana tested for SARS-CoV-2 infection between March 1 and December 31, 2020, linked to electronic health records. Primary measures were per capita rates of infection, hospitalization, and death. Age adjusted rates were calculated for multiple time periods corresponding to public health mitigation efforts. Comparisons across time within groups were compared using ANOVA.
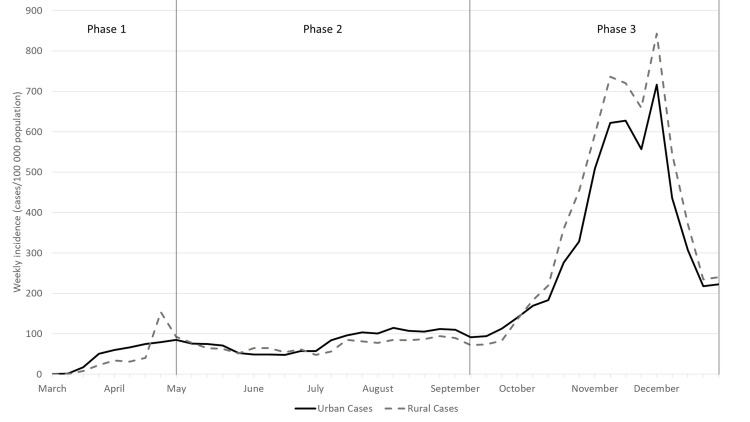
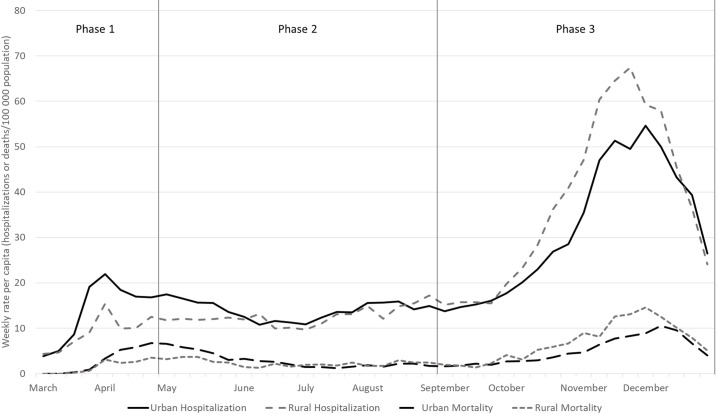
Results: Morbidity and mortality increased over time with notable differences among sub-populations. Initially, hospitalization rates among racial minorities were 3-4 times higher than whites, and mortality rates among urban residents were twice those of rural residents. By fall 2020, hospitalization and mortality rates in rural areas surpassed those of urban areas, and gaps between black/brown and white populations narrowed. Changes across time among demographic groups was significant for morbidity and hospitalization. Cumulative morbidity and mortality were highest among minority groups and in rural communities.
Conclusions: The synchronicity of disparities in COVID-19 by race and geography suggests that health officials should explicitly measure disparities and adjust mitigation as well as vaccination strategies to protect those sub-populations with greater disease burden.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Center for Systems Science and Engineering. COVID-19 Dashboard Baltimore: Johns Hopkins University; 2020 [cited 2020 Jul 19]. Available from: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594....
-
- Centers for Disease Control and Prevention US. COVIDView: A Weekly Surveillance Summary of U.S. COVID-19 Activity—Report for Week 52 Atlanta, GA: Department of Health and Human Services, U.S.; 2020. [updated Dec 26; cited 2021 Jan 5]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/pdf/covidview-01-04....
-
- Grasselli G, Zangrillo A, Zanella A, Antonelli M, Cabrini L, Castelli A, et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. Jama. 2020;323(16):1574–81. Epub 2020/04/07. doi: 10.1001/jama.2020.5394 ; PubMed Central PMCID: PMC7136855. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
