

Detection of circulating tumor DNA without a tumor-informed search using next-generation sequencing is a prognostic biomarker in pancreatic ductal adenocarcinoma
- PMID: 34298235
- PMCID: PMC8322473
- DOI: 10.1016/j.neo.2021.06.005
Detection of circulating tumor DNA without a tumor-informed search using next-generation sequencing is a prognostic biomarker in pancreatic ductal adenocarcinoma
Abstract
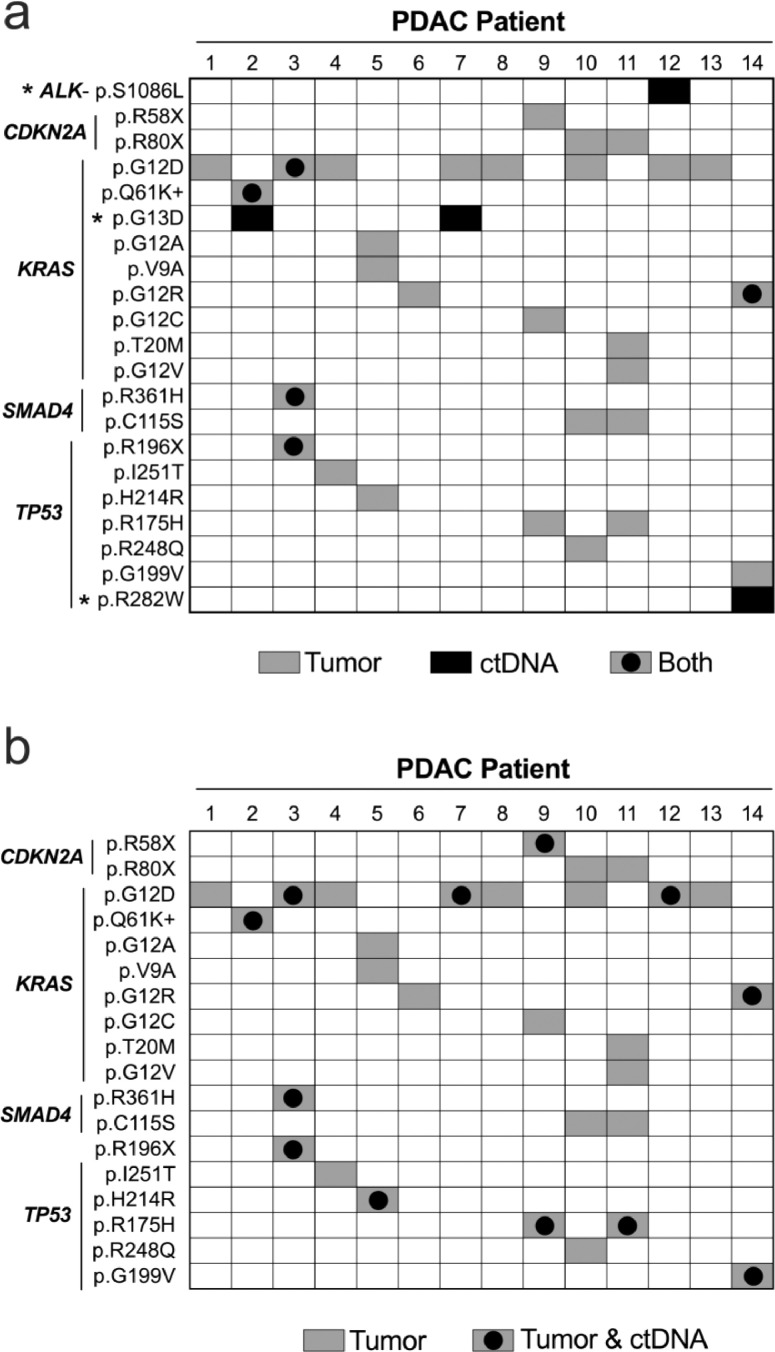
The confounding effects of next-generation sequencing (NGS) noise on detection of low frequency circulating tumor DNA (ctDNA) without a priori knowledge of solid tumor mutations has limited the applications of circulating cell-free DNA (ccfDNA) in clinical oncology. Here, we use a 118 gene panel and leverage ccfDNA technical replicates to eliminate NGS-associated errors while also enhancing detection of ctDNA from pancreatic ductal adenocarcinomas (PDACs). Pre-operative ccfDNA and tumor DNA were acquired from 14 patients with PDAC (78.6% stage II-III). Post-operative ccfDNA was also collected from 11 of the patients within 100 days of surgery. ctDNA detection was restricted to variants corresponding to pathogenic mutations in PDAC present in both replicates. PDAC-associated pathogenic mutations were detected in pre-operative ccfDNA in four genes (KRAS, TP53, SMAD4, ALK) from five patients. Of the nine ctDNA variants detected (variant allele frequency: 0.08%-1.59%), five had a corresponding mutation in tumor DNA. Pre-operative detection of ctDNA was associated with shorter survival (312 vs. 826 days; χ2=5.4, P = 0.021). Guiding ctDNA detection in pre-operative ccfDNA based on mutations present in tumor DNA yielded a similar survival analysis. Detection of ctDNA in the post-operative ccfDNA with or without tumor-informed guidance was not associated with outcomes. Therefore, the detection of PDAC-derived ctDNA during a broad and untargeted survey of ccfDNA with NGS may be a valuable, non-invasive, prognostic biomarker to integrate into the clinical assessment and management of patients prior to surgery.
Keywords: Biomarker; Cell-free DNA; Circulating tumor DNA; Next-generation sequencing; Pancreatic ductal adenocarcinoma.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Figures



References
-
- Sorenson GD, Pribish DM, Valone FH, Memoli VA, Bzik DJ, Yao SL. Soluble normal and mutated DNA sequences from single-copy genes in human blood. Cancer Epidemiol Biomarkers Prev. 1994;3:67–71. - PubMed
-
- Forshew T, Murtaza M, Parkinson C, Gale D, Tsui DW, Kaper F, Dawson SJ, Piskorz AM, Jimenez-Linan M, Bentley D. Noninvasive identification and monitoring of cancer mutations by targeted deep sequencing of plasma DNA. Sci Transl Med. 2012;4:136ra168. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
