

Definition of Outcome-Based Prostate-Specific Antigen (PSA) Thresholds for Advanced Prostate Cancer Risk Prediction
- PMID: 34298597
- PMCID: PMC8305281
- DOI: 10.3390/cancers13143381
Definition of Outcome-Based Prostate-Specific Antigen (PSA) Thresholds for Advanced Prostate Cancer Risk Prediction
Abstract
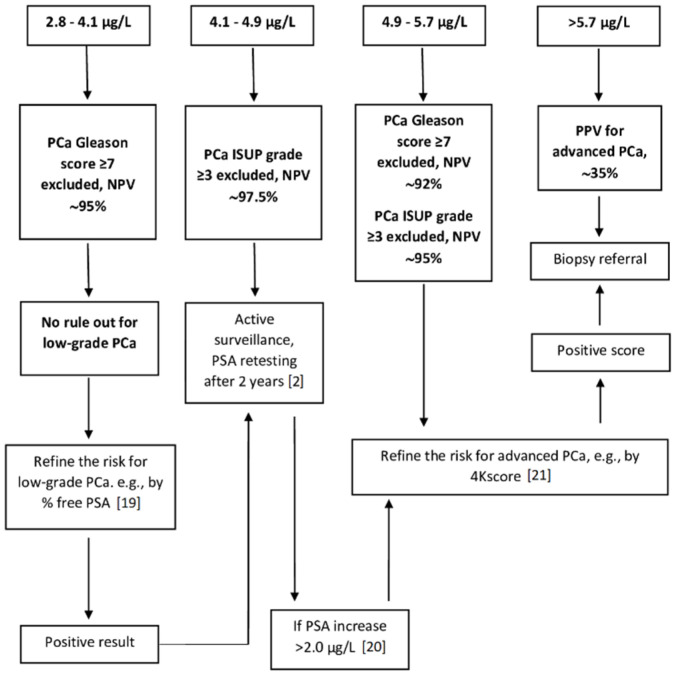
We defined prostate-specific antigen (PSA) thresholds from a well calibrated risk prediction model for identifying and excluding advanced prostate cancer (PCa). We retrieved 902 biopsied patients with a pre-biopsy PSA determination (Roche assay). A logistic regression model predictive for PCa including the main effects [i.e., PSA, age, histological evidence of glandular inflammation (GI)] was built after testing the accuracy by calibration plots and Hosmer-Lemeshow test for goodness of fit. PSA thresholds were derived by assuming a diagnostic sensitivity of 95% (rule-out) and 80% (rule-in) for overall and advanced/poorly differentiated PCa. In patients without GI, serum PSA concentrations ≤ 4.1 (<65 years old) and ≤3.7 μg/L (≥65 years old) excluded an advanced PCa (defined as Gleason score ≥ 7 at biopsy), with a negative predictive value of 95.1% [95% confidence interval (CI): 83.0-98.7] and 88.8% (CI: 80.2-93.9), respectively, while PSA > 5.7 (<65) and >6.1 μg/L (≥65) should address biopsy referral. In presence of GI, PSA did not provide a valid estimate for risk of advanced cancer because of its higher variability and the low pre-test probability of PCa. The proposed PSA thresholds may support biopsy decision except for patients with asymptomatic prostatitis who cannot be pre-biopsy identified.
Keywords: calibration; immunoassay; inflammation; prostate cancer; risk prediction.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Carter H.B., Albertsen P.C., Barry M.J., Etzioni R., Freedland S.J., Greeneet K.L., Holmberg L., Kantoff P., Konety B.R., Murad M.H., et al. Early detection of prostate cancer: AUA guideline. [(accessed on 29 April 2021)];J. Urol. 2013 190:419–426. doi: 10.1016/j.juro.2013.04.119. Available online: https://www.auanet.org/guidelines/prostate-cancer-earlydetection-guideline. - DOI - PMC - PubMed
-
- Gandaglia G., Albers P., Abrahamsson P.-A., Briganti A., Catto J.W., Chapple C.R., Montorsi F., Mottet N., Roobol M.J., Sønksen J., et al. Structured population-based prostate-specific antigen screening for prostate cancer: The European Association of Urology Position in 2019. Eur. Urol. 2019;76:142–150. doi: 10.1016/j.eururo.2019.04.033. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
