

Clinical and Imaging Features of Non-Small Cell Lung Cancer with G12C KRAS Mutation
- PMID: 34298783
- PMCID: PMC8304953
- DOI: 10.3390/cancers13143572
Clinical and Imaging Features of Non-Small Cell Lung Cancer with G12C KRAS Mutation
Abstract
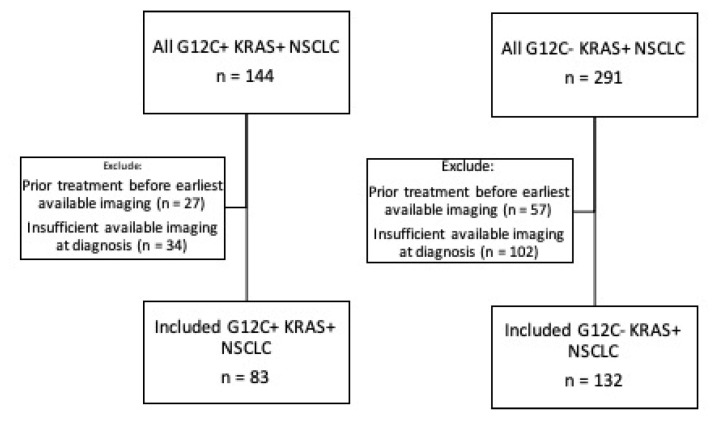
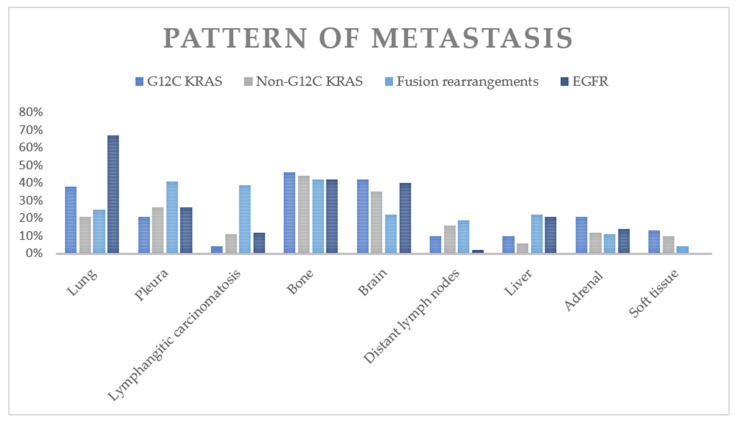
KRAS G12C mutations are important oncogenic mutations that confer sensitivity to direct G12C inhibitors. We retrospectively identified patients with KRAS+ NSCLC from 2015 to 2019 and assessed the imaging features of the primary tumor and the distribution of metastases of G12C NSCLC compared to those of non-G12C KRAS NSCLC and NSCLC driven by oncogenic fusion events (RET, ALK, ROS1) and EGFR mutations at the time of initial diagnosis. Two hundred fifteen patients with KRAS+ NSCLC (G12C: 83; non-G12C: 132) were included. On single variate analysis, the G12C group was more likely than the non-G12C KRAS group to have cavitation (13% vs. 5%, p = 0.04) and lung metastasis (38% vs. 21%; p = 0.043). Compared to the fusion rearrangement group, the G12C group had a lower frequency of pleural metastasis (21% vs. 41%, p = 0.01) and lymphangitic carcinomatosis (4% vs. 39%, p = 0.0001) and a higher frequency of brain metastasis (42% vs. 22%, p = 0.005). Compared to the EGFR+ group, the G12C group had a lower frequency of lung metastasis (38% vs. 67%, p = 0.0008) and a higher frequency of distant nodal metastasis (10% vs. 2%, p = 0.02). KRAS G12C NSCLC may have distinct primary tumor imaging features and patterns of metastasis when compared to those of NSCLC driven by other genetic alterations.
Keywords: KRAS mutation; lung cancer; radiology; targeted therapy.
Conflict of interest statement
M.Y.W., E.W.Z., D.P.M., L.L., J.K.L. and M.R.S.: None. J.F.G.: Consultant or received honoraria from Bristol-Myers Squibb, Genentech/Roche, Takeda, Loxo, Lilly, EMD Serono, Glyde Bio, Blueprint, Mirati, AstraZeneca, Pfizer, Novartis, Merck, Agios, Amgen, Helsinn, Regeneron, Oncorus, and Jounce, research support from Novartis, Genentech/Roche, and Ariad/Takeda, and institutional research support from Bristol-Myers Squibb, Tesaro, Moderna, Blueprint, Jounce, Array Biopharma, Merck, Adaptimmune, Novartis, and Alexo. Immediate family member who is an employee of Ironwood Pharmaceuticals. R.S.H.: Consulting honoraria from Boehringer Ingelheim, Novartis, Apollomics, Tarveda, Daichii Sankyo, EMD Serono. Research funding (to institution, not to self): Abbvie, Daichii Sankyo, Agios, Novartis, Corvus, Genentech/Roche, Mirati, Millenium, Exelixis, Celgene, Lilly. S.R.D.: Provides independent image analysis for hospital contracted clinical research trials programs for Merck, Pfizer, Bristol Mayer Squibb, Novartis, Roche, Polaris, Cascadian, Abbvie, Gradalis, Clinical Bayer, Janssen, Zai laboratories. Received honorarium from Siemens Healthineers (not related to work) and research funding from Lunit Inc.
Figures
References
-
- Forest F., Stachowicz M.-L., Casteillo F., Karpathiou G., Gouzy-Grosjean F., Guilaubey C., Cottier M., Beal J., Clemenson A., Péoc’H M. EGFR, KRAS, BRAF and HER2 testing in metastatic lung adenocarcinoma: Value of testing on samples with poor specimen adequacy and analysis of discrepancies. Exp. Mol. Pathol. 2017;103:306–310. doi: 10.1016/j.yexmp.2017.11.013. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
