

New Insights into Multiple Sclerosis Mechanisms: Lipids on the Track to Control Inflammation and Neurodegeneration
- PMID: 34298940
- PMCID: PMC8303889
- DOI: 10.3390/ijms22147319
New Insights into Multiple Sclerosis Mechanisms: Lipids on the Track to Control Inflammation and Neurodegeneration
Abstract
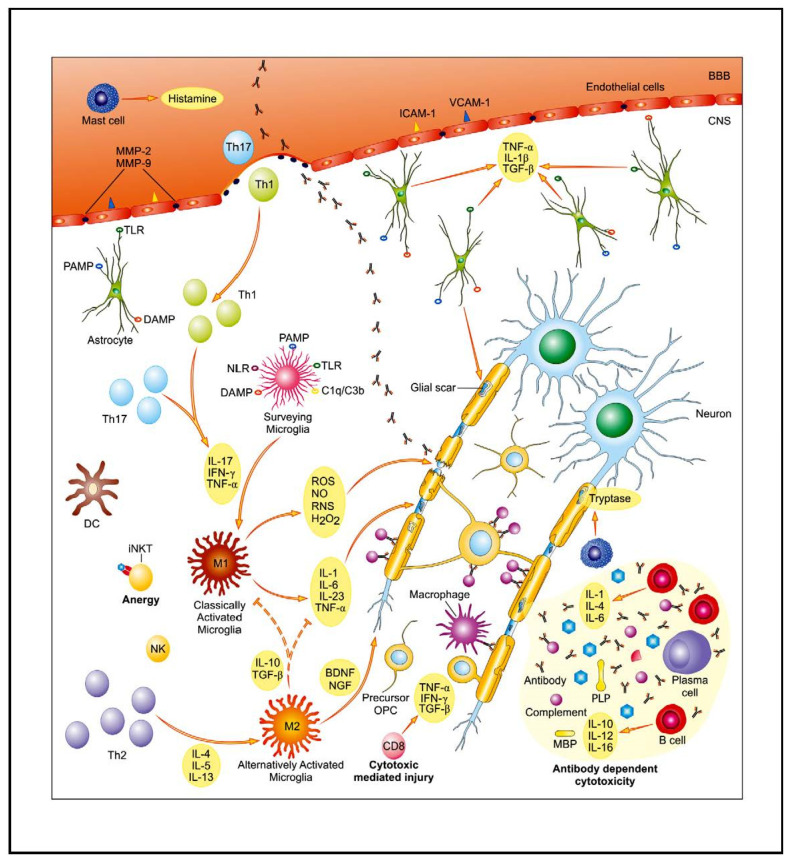
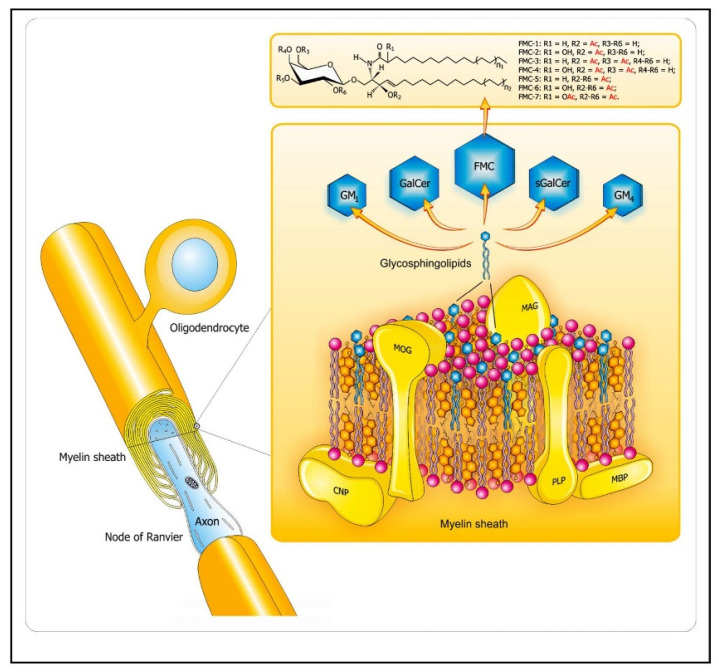
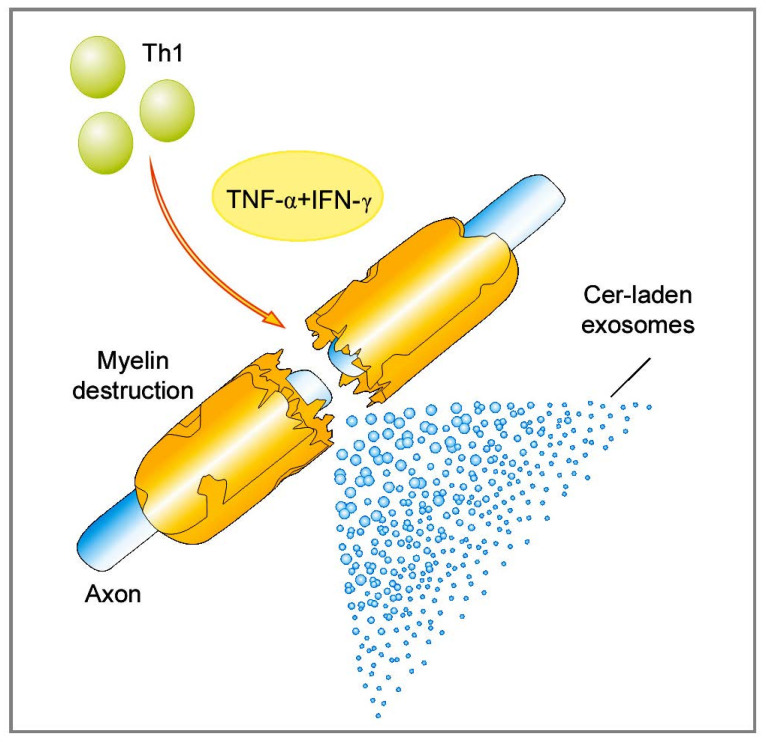
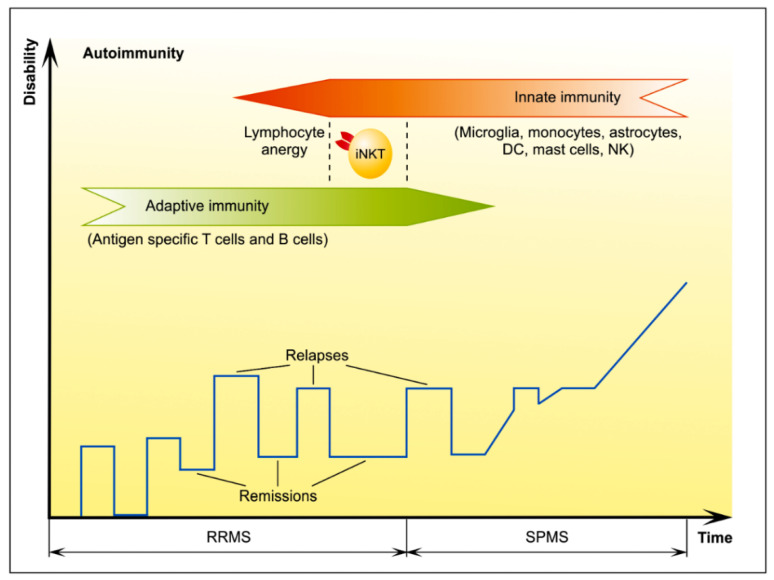
Multiple sclerosis (MS) is a central nervous system disease with complex pathogenesis, including two main processes: immune-mediated inflammatory demyelination and progressive degeneration with axonal loss. Despite recent progress in our understanding and management of MS, availability of sensitive and specific biomarkers for these both processes, as well as neuroprotective therapeutic options targeted at progressive phase of disease, are still being sought. Given their abundance in the myelin sheath, lipids are believed to play a central role in underlying immunopathogenesis in MS and seem to be a promising subject of investigation in this field. On the basis of our previous research and a review of the literature, we discuss the current understanding of lipid-related mechanisms involved in active relapse, remission, and progression of MS. These insights highlight potential usefulness of lipid markers in prediction or monitoring the course of MS, particularly in its progressive stage, still insufficiently addressed. Furthermore, they raise hope for new, effective, and stage-specific treatment options, involving lipids as targets or carriers of therapeutic agents.
Keywords: MS biomarkers; MS mechanisms; MS therapy; central nervous system; inflammation; lipidomics; lipids; multiple sclerosis; neurodegeneration; neurological diseases.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
